The human skull base houses some of the smallest and highest-contrast structures in the human body; high spatial resolution imaging is therefore critical to assessing its morphology and pathological processes.
Indeed, these characteristics make the skull base an ideal candidate for experimental flat-panel CT imaging, a fast-emerging technology that's coming soon to a radiology department near you.
In a study presented today at the European Congress of Radiology (ECR), researchers from Hannover Medical School in Germany compared flat-panel-based volume CT (fpVCT) to thin-section 16-row multidetector CT images of the whole human skull base. Flat-panel imaging beat 16-slice MDCT hands down in a subjective visualization of 21 structures in the skull base.
Multidetector CT has limitations when imaging such tiny structures, and would clearly benefit from higher resolution, said Dr. Sönke Bartling from the department of neuroradiology at the University of Hannover in Germany.
The geometry of conebeam CT, together with the smaller size of the flat-panel detectors, makes for higher-resolution images with flat-panel volume CT that could potentially improve image interpretation. However, "the drawback of flat-panel CT is low soft-tissue contrast and very long scan times," Bartling said.
To date flat-panel conebeam scanners have produced impressive results in small imaging experiments of individual bones, such as a human temporal bone, he said. But scanning a larger chunk of anatomy, such as an entire skull base, with flat-panel-detector-based CT presented a greater challenge due to greater beam scatter and potentially higher dose for the acquisition.
Thus the study examined scans of three embalmed human cadaver heads with both MDCT (LightSpeed 16, GE Healthcare, Chalfont St. Giles, U.K.) and the investigational GE flat-panel volume CT (fpVCT) scanner.
First, thin-section MDCT scanning was performed to optimize spatial resolution (120 kV, 80 mA, and 0.625-mm collimation), reconstructed at 9.6-cm fFOV, 512 x 512 matrix, and 0.3-mm z-spacing with a bone window.
The step-and-shoot fpVCT scan protocol consisted of 1,000 projections, eight-second rotation, 140 kVp, and 25 mAs, with a modified FDK (Feldkamp, Davis, and Kress) conebeam reconstruction algorithm.
To compare the results, two independent readers rated the appearance of 21 structures of the skull base and maxillofacial region on a four-point scale. Rated structures included:
Temporal bone
- Bone marrow cavity of incus
- Incudomalleolar joint
- Incudostapedial joint
- Lenticular process of incus
- Head of stapes
- Anterior crus of stapes
- Posterior crus of stapes
- Footplate of stapes
- Stapedius muscle
- Vestibular aqueduct
- Cochlear aqueduct
- Bony wall of facial nerve (middle ear)
- Tendon of tensor tympani
- Canal of cochlear nerve
- Gap between stapes footplate and ovale window niche
- Osseus spiral lamina in cochlea
Central skull base
- Canal of greater petrosal nerve
- Pterygoid (vidian) canal
Frontal skull base/maxillofacial region
- Canal of n. opticus
- Canal of anterior alveolar nerve
- Canal of olfactory nerve branch in cribiform plate
The fpVCT scanner consists of two flat-panel detectors (10242 elements at 2002 µm2) mounted side by side on a standard CT gantry. The scan field-of-view was 33 cm, with 3.4-cm z-coverage per rotation of 3.4 cm.
Both modalities produced diagnostic images, but fpVCT produced a significantly higher average sum score (60.8) compared to MDCT (41.5) (p < 0.02). In particular, structures such as the stapedial muscle and the bony walls of the facial nerve canal were much more clearly displayed in fpVCT, Bartling said.
 |
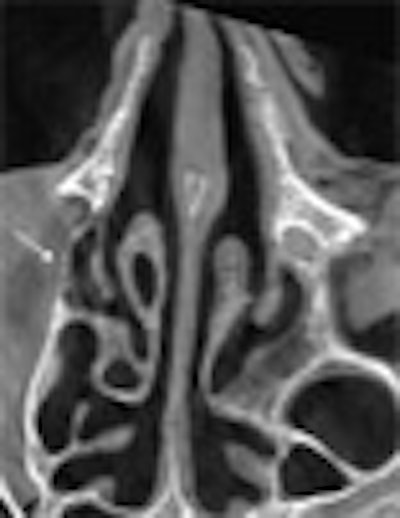
| The flat-panel VCT images of the skull base at right were rated significantly higher in image quality compared to 16-slice MDCT images of the same regions at left, by two readers rating 21 features independently. Images (from top to bottom) include stapes and ovale window niche (above), facial nerve canal (below), maxillofacial region, and implanted microscrews (bottom). All images courtesy of Dr. Sönke Bartling. |
 |
 |
 |
"The same holds true for small and especially thin structures within the maxillofacial region, for example the medial limitation of the orbital cavity is much better delineated in flat-panel-based volume CT," Bartling said. And the technique produces fewer metal artifacts, he added.
"Flat-panel volume CT of the whole human skull base is possible, and we have better delineation of small high-contrast structures and thin high-contrast structures, and improvement is possible in surgical planning, navigation and maybe diagnostic imaging," Bartling concluded.
In response to a question from the audience, Bartling said that the radiation dose was not meaured for this particular experiment, but is roughly equivalent to a normal MDCT bone scan for the protocols used. This is possible because flat-panel systems essentially trade off higher resolution for higher noise, he said.
By Eric Barnes
AuntMinnie.com staff writer
March 7, 2006
Related Reading
AuntMinnieTV: German group investigates '1,024-slice' CT, May 6, 2005
CT is the blanket modality for neuroimaging blunt injury patients, January 12, 2006
MDCT answers most head and neck questions, November 18, 2005
Copyright © 2006 AuntMinnie.com















