Thirty years after breast CT was introduced, abandoned, and then reintroduced, California researchers believe they have a viable breast CT unit that may detect tumors sooner than mammography. The group presented the results of their most recent research Sunday at the American Association of Physicists in Medicine (AAPM) meeting in Seattle.
"We have built a dedicated CT scanner to produce volumetric images of the breast and begun a preliminary clinical trial in volunteers and selected patients," according to the group's AAPM abstract. Thomas Nelson, Ph.D., from the University of California, San Diego, presented the 3D CT breast images at the meeting. His co-authors include John Boone, Ph.D., and J. Anthony Siebert, Ph.D., both from the University of California, Davis in Sacramento. A description of the prototype CT scanner can be found in a 2001 article in Radiology (December 2001, Vol. 221:3, pp. 657-667).
For the current study, the group set out to evaluate visualization and identification of breast glandular tissue patterns in breast CT volume data and whether it had potential to improve lesion detection.
Imaging was performed using 80 kVp doses, which is comparable to a standard two-view mammogram. On this prototype scanner, the exam took about 17 seconds per breast. The total exam time was equal to, or slightly quicker, than a standard mammogram, Boone told AuntMinnie.com.
"In mammography, the breasts are positioned four times. In breast CT, (they are positioned) twice, so our experience is that ... 15 minutes is all that it takes," Boone explained in an e-mail. Boone is the vice chairman of research of radiology and a professor of biomedical engineering at the Davis medical center.
 |
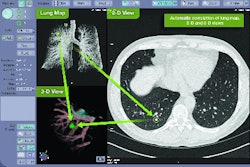
| The breast CT scanner developed at the UC Davis School of Medicine and Medical Center produces about 300 individual images per breast. Image courtesy of UC Davis Health System. Copyright 2005 UC Regents. All rights reserved. |
A modified Feldkamp algorithm was used to reconstruct the images. The breast CT data of 512^ 3 voxels had an isotropic resolution of about 300 µm. The volume data were analyzed and viewed on a specially designed workstation. The data were displayed using blending, maximum intensity projection (MIP), and summation projection algorithms. Breast glandular structures were identified based on CT number, voxel histograms, and structural features.
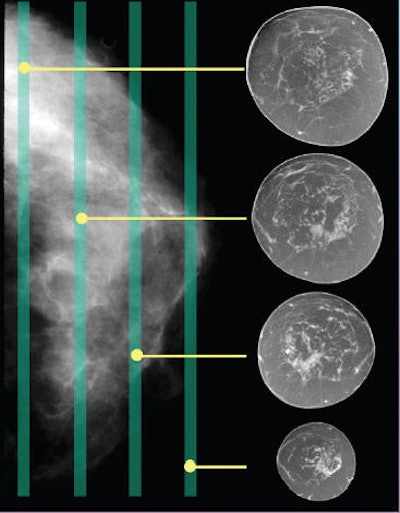
According to the results, the breast CT images "showed impressive breast parenchyma and glandular structure detail with excellent contrast resolution." The authors stated that summation projection and thick slices provided optimal viewing of ductal structures. Multiplanar slices permitted rapid scrolling. Voxel CT numbers, histograms, and architectural features were useful for differentiating glandular tissue from fat, skin, and connective tissues. The MIP images demonstrated calcifications.
"Voxel CT numbers plus direct interactive viewing provided the mammographer (with) clearer views of breast architecture and glandular tissues," the group concluded. "Workstation display flexibility presented data appearing similar to mammograms plus additional tomographic slices further enhancing conspicuity of breast architecture."
For the next phase, the group plans to test breast CT in a clinical trial with about 190 patients. The trial will be open to UC Davis patients with recent mammograms that are suspicious for breast cancer. Trial participants will undergo breast CT followed by biopsy, if necessary.
If the trial shows that breast CT is as effective as mammography for tumor detection, the next step will be a larger trial to determine whether the new technology can indeed detect tumors earlier than mammography. This extensive trail could be under way within three years, according to Boone.
"CT became clinical in 1972, and images were really pretty bad in the 1970s and early 1980s, due to the detector/scanner technology and the basic algorithms available in that era," Boone stated. "Our (current) voxel volume is 200 times smaller than that early breast scanner so our spatial resolution is far, far better. I believe that our contrast resolution is also better because of the better detector technology available to us today, compared to 30 years ago."
For the first phase of the trial, all CT images will be read by qualified radiologists, as well as some senior radiology residents. Boone explained how reading a breast CT differs from reading a screening mammogram.
"The breast CT dataset has 300 images (could be more), and thus stack mode is used. We have developed software which simultaneously displays the three orthogonal views -- sagittal, coronal, and axial," he stated. "Lots of work remains in terms of optimizing the radiologist interface to the volume dataset, but we have a feature-rich visualization package specifically for breast CT.... The biggest difference is that the radiologist really needs to work with the volume dataset in breast CT, whereas (mammograms) are read with relatively static display."
The breast CT scan may also address two common complaints that women lodge about screening mammography -- discomfort during the exam and anxiety while waiting for the results.
Thus far, women who have undergone tests on the CT scanner have not complained of discomfort, mostly because breast CT does not require compression (although immobilization may be required), Boone noted, adding that his group is working to optimize the design of the table and make the back, neck, and arm positions more comfortable.
In terms of the wait time for results, it will depend more on how the images are read rather than the modality used. "The waiting ... is more a consequence of how a particular breast imaging clinic functions (end-of-day batch reading, for example, versus on-the-fly, contemporaneous reading before the patient leaves the clinic), and that will not change between breast CT and (mammography). We certainly don't think that reading the breast CT images will be any faster, but (computer-aided detection) may change that in time," Boone explained.
Finally, the trial will address reproducibility issues as well as ease-of-use with breast CT, particularly for the technologists who are doing the patient positioning. To date, the group has scanned 24 women, of which there were two or three cases of breath-related motion artifacts.
"We are still working on optimizing table design for better imaging into the chest wall and axilla. Other than these issues, positioning is relatively straightforward. We will be adding things like laser beams to help this soon," Boone stated.
By Shalmali Pal
AuntMinnie.com staff writer
July 25, 2005
Related Reading
UC Davis tests breast CT, May 11, 2005
Routine chest CT does double duty for breast imaging, July 3, 2001
Dedicated breast CT delivers low radiation dose, fine architectural detail, November 28, 2000
Copyright © 2005 AuntMinnie.com