It took a difficult and time-consuming study of animals, specifically pigs, to compare multidetector-row CT to MRI for left ventricular (LV) function assessment in the setting of acute myocardial infarction (MI). But the illuminating results showed that MDCT was largely equivalent to gold-standard MRI for determining left ventricular volumes and assessing wall motion.
Still, the 16-slice CT images fell significantly short of MRI in assessing the more time-dependent functional parameters, the group concluded, suggesting that the next generation of MDCT scanners could potentially close the gap.
The study began in an effort to determine whether myocardial infarction could be visualized in late myocardial enhancement with multislice spiral CT as well as MRI, said lead investigator Dr. Andreas Mahnken from Aachen University of Technology in Aachen, Germany. His coinvestigators were Drs. Marcus Kathoh, Elmar Spuentrup, Joachim Wildberger, Rolf Günther, and Arno Bücker.
"We performed ... balloon occlusion of the left anterior descending (LAD) branch of the left artery," Mahnken said in a presentation at the 2005 European Congress of Radiology (ECR) in Vienna, Austria. "And of course we had some complications -- you can't (induce) myocardial infarction in animals without any problems. We had to perform electromechanical defibrillation in seven animals, and one of them died."
The experiment was conducted on 15 pigs (53.9 ± 9.5 kg, heart rate 88.9 ± 12.0 bpm) under general anesthesia. Following LAD occlusion and defibrillation when needed, the animals underwent MR imaging on a 1.5-tesla Gyroscan Intera MRI scanner (Philips Medical Systems, Andover, MA). Twenty-five heart phases were acquired at TR 3.1 sec, TE 1.6 msec, flip angle of 60 degrees, 350 x 270-mm2 field-of-view, 256 x 152 matrix, and temporal resolution of 32 msec, he said.
Next, cardiac MDCT images were acquired on a Sensation 16 (Siemens Medical Solutions, Erlangen, Germany) following administration of 12 mL of Ultravist 370 (Schering, Berlin) at 12 x 0.75 mm, 120 kVp, 500 mAs, using collimation of 1 mm, field-of-view of 180 mm, and B30f kernel.
"Typical image reconstruction parameters were chosen, and we also calculated 20 phases just to get temporal resolution at best (0-95%, temporal resolution 105-210 msec)," Mahnken said. "Short-axis and long-axis slices were reconstructed at multiplanar reformats from the data. Thereafter we started with a functional analysis from the short-axis MPRs, 8-mm slice thickness, in a well-established sequence on our scanner so we used the same slice thickness for the (MDCT). No interslice gap was chosen."
Two radiologists evaluated the myocardium by consensus using 2002 American Heart Association guidelines. They calculated LV volumes (end-diastolic volume, end-systolic volume, stroke volume), peak filling rate (PFR), peak ejection rate (PER), time to PER (TPER), and time from end-systole to PFR (TPFR), as well as myocardial mass, from manually drawn end and epicardial contours.
They visually assessed regional wall motion from cine loops, and analyzed LV function using the Bland-Altman method, Student's t-test analysis, and Pearson's correlation coefficient.
 |
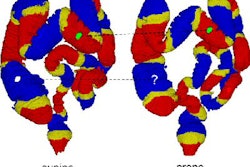
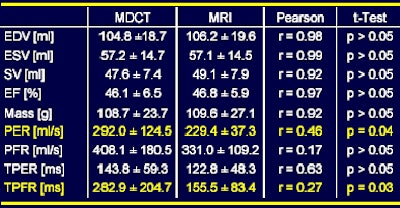
| The results show good correlation between CT and MRI in LV volumes, but poor correlation in the more time-dependent PER, PFR, TPER, and TPFR parameters. Chart and data courtesy of Dr. Andreas Mahnken. |
Regional wall motion was visually assessed from cine loops, and segments classified as akinetic, hypokinetic, or normal, Mahnken said. LV function was analyzed using the Bland-Altman method, Student's t-test, and Pearson's correlation coefficient. Regional wall motion scores were compared with weighted kappa statistics.
MDCT and MRI results were well-correlated for LV volumes, Mahnken said. The mean ejection fraction (EF) was 46.1 ± 6.5% on MDCT and 46.8 ± 5.9% on MR imaging (r = 0.97), and no systematic errors were seen on the Bland-Altman analysis. Regional wall motion scores demonstrated a very high level of agreement between both modalities with a kappa value of 0.878.
But the results for PER, PFR, TPER, and TPFR parameters were markedly worse, yielding a wide range of scattering and significant differences between MRI and MDCT for PER (p = 0.04) and TPFR (p = 0.03).
Sixteen-detector CT allows for reliable assessment of LV volumes and regional wall motion at rest, but is not yet suited for the assessment of functional parameters that directly depend on temporal resolution.
"From our data we concluded that multislice CT allows for visual assessment of the wall motion and, of course, allows calculation of left ventricular volumes," Mahnken said. "But it's not yet suited for the assessment of directly time-dependent parameters (such as PER or TPFR) and (MDCT) was very time-consuming. So you really have to think about if you want to do it."
The use of a 64-detector MDCT scanner could potentially close the gap with MRI, he said.
By Eric Barnes
AuntMinnie.com staff writer
June 29, 2005
Related Reading
MDCT maybe equivalent to MRI, tops echo and SPECT for heart function, February 15, 2005
Cardiac MR center finds success with 'one-stop shopping' model, January 25, 2005
Left ventricular hypertrophy accompanies obesity in young, healthy women, April 23, 2004
Coronary MS CTA quantifies LV function adequately, March 23, 2004
MR tagging identifies LV torsion-to-shortening ratio in AS, March 4, 2004
Copyright © 2005 AuntMinnie.com