AI assistance can improve the detection accuracy of thoracic abnormalities on chest x-rays across radiologists with varying levels of expertise, according to a study published December 12 in Radiology.
In a retrospective study, a commercially available algorithm (ChestView, v. 1.2.0, Gleamer) increased sensitivity for detecting all abnormalities on x-rays for all readers (thoracic radiologists, general radiologists, and radiology residents), according to a group of Gleamer consultants and clinicians at Cochin Hospital in Paris.
“Our findings suggest that artificial intelligence assistance in chest radiograph interpretation may enhance sensitivity without affecting specificity for all readers, regardless of their level of expertise or seniority or the type of abnormality,” wrote first author Souhail Bennani, MD, and colleagues.
Chest x-ray remains the most common radiologic examination worldwide and interpretation of its results can be difficult, the authors explained. Thus, in this study, they explored the potential benefit of AI assistance in detecting five thoracic abnormalities by evaluating the performance of radiologists with different levels of expertise, both with and without AI assistance.
The group gathered 500 images from patients who underwent both chest x-ray and thoracic CT within 72 hours at their hospital between January 2010 and December 2020. About 50% of the x-rays had abnormal findings. A senior thoracic radiologist annotated all images for five abnormalities (pneumothorax, pleural effusion, consolidation, mediastinal and hilar mass, and lung nodule) based on the corresponding CT results, which served as the ground truth.
Next, a total of 12 readers (4 thoracic radiologists, 4 general radiologists, 4 radiology residents) read half the x-rays without AI and half with AI, with changes in sensitivity and specificity then calculated.
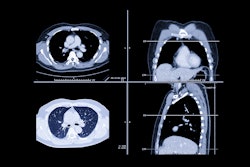
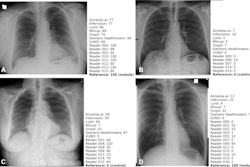
 AI detected a lung mass, a lung nodule, and a small pneumothorax. Without AI assistance, only one thoracic radiologist and one general radiologist detected all abnormalities, whereas with AI assistance, one thoracic radiologist, two general radiologists, and one resident detected all abnormalities. Corresponding coronal and axial CT images show the lung mass (arrows), the lung nodule (white arrowheads), and the small pneumothorax (black arrowheads) that should have been detected on the chest radiograph. Image courtesy of Radiology.
AI detected a lung mass, a lung nodule, and a small pneumothorax. Without AI assistance, only one thoracic radiologist and one general radiologist detected all abnormalities, whereas with AI assistance, one thoracic radiologist, two general radiologists, and one resident detected all abnormalities. Corresponding coronal and axial CT images show the lung mass (arrows), the lung nodule (white arrowheads), and the small pneumothorax (black arrowheads) that should have been detected on the chest radiograph. Image courtesy of Radiology.
According to the findings, on average for all readers, AI use resulted in an absolute increase in sensitivity of 26% for pneumothorax, 14% for consolidation, 12% for nodules, 8.5% for pleural effusion, and 5.9% for mediastinal and hilar masses.
In addition, the mean reading time was 81 seconds without AI versus 56 seconds with AI (a 31% decrease, p < 0.001), the authors reported.
Ultimately, focusing on five abnormalities rather than analyzing every possible abnormality on a chest x-ray does not represent clinical practice scenarios, nor were the radiologists aware of the clinical indication or patient’s medical history, which also would have reflected daily practice, the authors noted.
“Prospective evaluation in clinical practice with a natural prevalence of abnormal conditions should be considered to confirm these benefits,” the group concluded.
The full study is available here.