A new chest x-ray technique implemented during the COVID-19 pandemic of imaging patients through glass produced diagnostic-quality radiographs while reducing hospital costs and infection risk, according to an April 7 paper in the Journal of Medical Imaging and Radiation Sciences.
A team at St. Michael's Hospital in Toronto implemented a "through glass" chest x-ray (TG-CXR) technique recommended by the RSNA's COVID-19 task force. The group found the method saved more than $51,000 in a year while reducing the associated risk of infection for staff performing the scans, according to first author Dr. Tian Yang Liu and colleagues from the University of Toronto.
The COVID-19 pandemic has posed many unprecedented challenges to the healthcare system. Foremost amongst these is the challenge of safeguarding the health and safety of healthcare personnel in the face of worldwide shortages of personal protective equipment (PPE), according to the authors. Finding innovative ways to minimize front-line worker exposure and conserve PPE, while not sacrificing the quality of patient care, is therefore crucial in the global efforts to suppress this disease, they wrote.
To that end, Liu et al sought to understand the cost and benefit in quantifiable terms of adopting TG-CXR for COVID-19 patients.
The TG-CXR method involves having only one technologist don PPE and enter the isolation room to position the patient and cassette/detector. A second technologist stays with the portable x-ray machine outside of the isolation room. Once the patient is in a satisfactory position, the first technologist provides breathing instructions to the patient and then signals the second technologist to trigger the exposure. While the first technologist waits in the isolation room, the second confirms that the acquired image is of satisfactory quality.
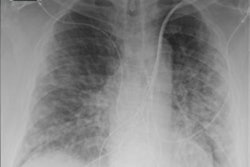
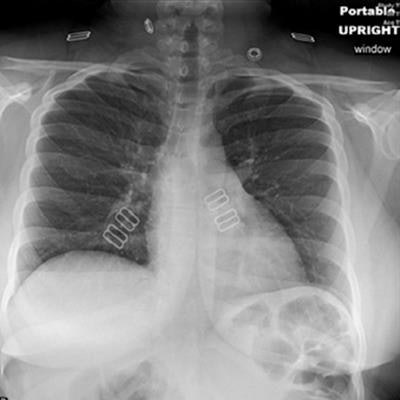
 Chest radiography through glass. (A) A technologist positions the portable radiography unit outside the patient room with the x-ray tube facing the wire-reinforced isolation room window. (B) Anteroposterior chest radiograph obtained through glass is of diagnostic quality. Images courtesy of the RSNA.
Chest radiography through glass. (A) A technologist positions the portable radiography unit outside the patient room with the x-ray tube facing the wire-reinforced isolation room window. (B) Anteroposterior chest radiograph obtained through glass is of diagnostic quality. Images courtesy of the RSNA.Importantly, since the portable radiography machine was never in the patient's room, it does not require cleaning, the authors noted.
To assess the technique, Liu et al performed a study of 316 chest radiographs obtained using the TG-CXR method during the study period, an average of 14.4 imaging studies each day. Technologists were trained on the method during a 15-minute shift-change briefing. This translated to a one-time cost of $424.88. There was an average reduction of portable radiography machine downtime of four minutes and 48 seconds per study. The benefit of adopting the TG-CXR technique was $9.87 per patient. This resulted in a projected net cost savings of $51,451.84 per year.
| Benefit of through-glass chest x-ray for COVID-19 patients | |||
| Per radiograph | 1 year | 5 years | |
| Dollar saving from PPE conservation | $3.54 | $18,606.24 | $93,031.20 |
| Dollar savings from sanitization material | $0.54 | $2,838.24 | $14,191.20 |
| Portable x-ray machine downtime reduction | 4 min, 48 sec | 112 hrs, 14 min, 24 sec | 561 hrs, 12 min, 0 sec |
| Reduction of technologist cost | $5.79 | $30,432.24 | $152,161.20 |
| Net benefit | $9.87 | $51,876.72 | $259,383.60 |
In addition to the cost savings, the through-glass chest x-ray technique decreased the number of staff exposed to patients who are suspicious for or confirmed of having COVID-19, which resulted in decreased risk of transmission and provided an important advantage during the fight against the current pandemic.
Other benefits that could not be quantified include a potential decrease in sick leave, employee healthcare costs, and psychological stress from decreased risk of transmission, as well as a potential reduction in administrative time, and the effort and cost required to procure adequate PPE supplies.
The authors noted, however, that the study was limited in that they only used data from a single institution. They also added that not all hospitals are built with glass partitions between patient rooms and staff areas and, thus, the through-glass technique may not be universally implementable.
In the future, the through-glass chest x-ray technique may be expanded to include imaging studies other than chest radiography (such as abdomen and extremity imaging), yielding increased cost savings. The ease of implementation and cost savings associated with instituting the TG-CXR technique makes a strong argument for its continuation in the post-COVID-19 pandemic era.
"We hope that our findings would encourage policy-makers to implement TG-CXR techniques at their institutions when and where possible," Liu and colleagues concluded.