Prioritizing which women receive breast screening based on their risk factors could enable breast centers to focus on the patients who need screening most during backlogs such as what occurred during the COVID-19 pandemic according to a study published March 25 in JAMA Network Open.
The study of 1.9 million women and five years of data from breast registries connects risk factors such as a personal history of breast cancer or a referral for a diagnostic exam to evaluate a lump with breast cancer detection rates.
Researchers found many more cancers in individuals who were at higher risk for getting a positive result based on risk factors. In fact, 12.1% of the mammography volume came from high-risk or very-high-risk patients, but these individuals accounted for 55% of all breast cancers detected.
By comparison, women at lowest risk for cancer, such as individuals between the ages of 50 and 69 undergoing annual screening, accounted for 44.2% of volume but only 13.1% of detected cancers, wrote a team led by Diana Miglioretti, PhD, professor and division chief of biostatistics, at the University of California, Davis.
The study explored the use of risk stratification modeling to guide patient selection during the pandemic, which forced a shift away from care deemed to be nonessential. Miglioretti and colleagues noted that the COVD-19 pandemic results in a "precipitous drop" in screening that likely reduced the number of breast cancers diagnosed.
"As COVID-19 case rates continue to increase in waves, radiology facilities face significant scheduling challenges in addressing the backlog of postponed mammograms, reduced staff, and reduced number of mammogram appointment times required to maintain physical distancing and safety protocols, resulting in markedly diminished imaging availability," they noted.
Could triaging individuals for screening help centers cope with the backlog? To answer the question, researchers examined data that had been prospectively collected between 2014 and 2019 by seven Breast Cancer Surveillance Consortium (BCSC) registries in the U.S. Nearly 1.9 million mammograms were included in the analysis.
Out of all the mammograms reviewed, approximately 1.7 million were performed on individuals with no personal history of breast cancer, most of which were performed for breast cancer screening. Overall, the cancer detection rate was 11.5 per 1,000 mammograms, compared with 18.6 per 1,000 for those with a personal history of breast cancer.
Patients considered at moderate risk for cancer included those with a history of a high-risk lesion or a diagnosis of breast cancer longer than 10 years ago. Low-risk groups included patients with a more recent past diagnosis of breast cancer and those ages 50-59 undergoing annual screening.
| Cancer detection rate based on breast cancer risk | ||
| Risk group | Indication for evaluation | Number of cancers detected per 1,000 mammograms |
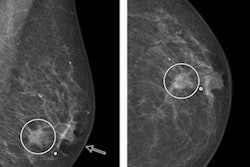
| Very high risk | Abnormal mammogram or lump, with personal history of breast cancer | 122.3 |
| Abnormal mammogram or lump, no personal history | 89.6 | |
| High risk | Short-interval follow-up or evaluation for symptoms other than lump, with personal history | 47.5 |
| Symptoms other than lump, with personal history | 40.9 | |
| Abnormal mammogram or lump, no history of breast cancer | 36.1 | |
The authors urged the development of infrastructure and resources to allow the implementation of risk-based scheduling, taking patients' preferences and coronavirus risks into account.
In an editorial also published March 25 in JAMA Network Open, Northwestern University radiologists Drs. Sarah Friedewald and Dipti Gupta noted that the criteria used in the study to triage women might identify more cancers in some risk groups than the traditional use of a binary system -- screening or diagnostic -- to categorize patients.
Indeed, the current study produced the counterintuitive finding that the cancer detection rate for screening mammograms can be higher than diagnostic mammograms: The rate for those with a high-risk lesion and no personal history of breast cancer was 12.7 per 1,000 compared with 7.3 per 1,000 in those younger than 70 with a personal history of breast cancer who underwent a follow-up diagnostic study for a probably benign finding, they pointed out.
The authors also noted that the American College of Radiology and the American College of Breast Surgeons had recommended postponing screening until the pandemic was under control.
"Triaging mammographic examinations based on screening and diagnostic examination types seems more efficient and attainable," they wrote.