PET/MRI scans with a gallium-68 (Ga-68)-labeled radiopharmaceutical that homes in on prostate-specific membrane antigen (PSMA)-11 could become a mainstay in prostate cancer detection, given its ability to significantly outperform multiparametric MRI alone, according to a study published online September 18 in Radiology.
Ga-68 PSMA PET/MRI was significantly more proficient in detecting tumors in patients, leading to significantly greater sensitivity than multiparametric MRI. Researchers from the University of California, San Francisco (UCSF) also used two unique approaches to find the locations of positive tumor regions, which also confirmed the findings.
"Our findings may improve the diagnostic confidence of radiologists when evaluating patients referred for imaging after a positive biopsy result," wrote the researchers, led by Dr. Robert Hicks from UCSF's department of radiology and biomedical imaging. "Radiologists will then be able to risk-stratify patients as having a high likelihood of clinically significant prostate cancer and identify appropriate candidates for definitive therapy."
The retrospective study included 32 patients (median age, 68 years; range, 62-71 years) with biopsy-proven prostate cancer who underwent preoperative staging with simultaneous Ga-68 PSMA-11 PET, whole-body time-of-flight MRI, and multiparametric MRI of the prostate before radical prostatectomy between December 2015 and June 2017.
Scans were performed on a 3-tesla time-of-flight (TOF) PET/MRI system (Signa, GE Healthcare). Patients were imaged for a mean period of 71 minutes (± 14 minutes) after intravenous injection of Ga-68 PSMA-11 at a mean of 210.9 MBq (± 44.4 MBq).
Image acquisition was divided into two segments. The first sequence included a dedicated 15-minute scan of the pelvis with TOF-PET data reconstruction with 28 subsets. The second phase consisted of whole-body PET/MRI with three minutes of PET acquisition at each bed position for pelvic images.
The researchers based tumor localization on 30 anatomic regions and calculated sensitivity and specificity based on raw stringent and alternative neighboring approaches. With the raw stringent approach, radiologic and pathologic data were confirmed when a tumor was present in the same region. With the alternative neighboring approach, results were based on detection of a tumor in the same region or any of the immediately adjacent regions.
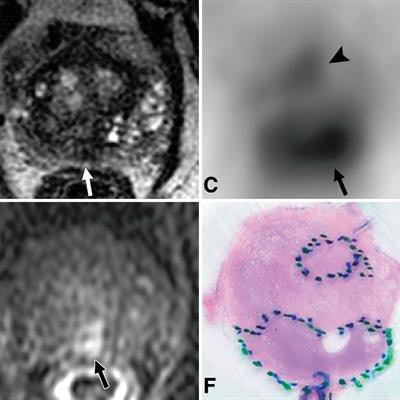
 Images are from a 72-year-old man with prostate-specific antigen level of 5.9 ng/mL. Axial diffusion-weighted MR image (A) of midprostate and corresponding apparent diffusion coefficient map (D) demonstrate a single focus of restricted diffusion (arrow) in the midline posterior peripheral zone. The focus (arrow) has ill-defined low signal intensity on the T2-weighted MR image (B) and suspicious enhancement (E) on the dynamic T1-weighted postcontrast image. Corresponding PET scan (C) shows two separate areas of focal radiotracer uptake, including one focus in midline posterior peripheral zone with maximum standardized uptake value (SUVmax) of 11.7 (arrow) and an additional focus in the central aspect of the left anterior peripheral zone with an SUVmax of 6.2 (arrowhead). Histopathologic slide of midprostate (F) confirms the presence of two distinct tumors. Images courtesy of Radiology.
Images are from a 72-year-old man with prostate-specific antigen level of 5.9 ng/mL. Axial diffusion-weighted MR image (A) of midprostate and corresponding apparent diffusion coefficient map (D) demonstrate a single focus of restricted diffusion (arrow) in the midline posterior peripheral zone. The focus (arrow) has ill-defined low signal intensity on the T2-weighted MR image (B) and suspicious enhancement (E) on the dynamic T1-weighted postcontrast image. Corresponding PET scan (C) shows two separate areas of focal radiotracer uptake, including one focus in midline posterior peripheral zone with maximum standardized uptake value (SUVmax) of 11.7 (arrow) and an additional focus in the central aspect of the left anterior peripheral zone with an SUVmax of 6.2 (arrowhead). Histopathologic slide of midprostate (F) confirms the presence of two distinct tumors. Images courtesy of Radiology.Overall, Ga-68 PSMA-11 PET/MRI depicted prostate cancer in 31 patients (97%), compared with 79% with multiparametric MRI (23 of 29 patients with conclusive multiparametric MRI examinations).
The histopathologic exams detected 412 positive tumor regions (43%) among 960 total regions in the 32 patients. By comparison, Ga-68 PSMA-11 PET/MRI depicted a few more positive tumor regions -- 434 regions (45%) -- while multiparametric MRI found 287 positive regions (30%).
In assessing the raw stringent and alternative neighboring approaches, Ga-68 PSMA-11 PET/MRI significantly exceeded multiparametric MRI for sensitivity in both cases (p < 0.001). As for specificity, Ga-68 PSMA-11 PET/MRI was significantly less than multiparametric MRI with the raw stringent approach but similar with the alternative neighboring approach (p = 0.99).
| MRI vs. Ga-68 PSMA-11 for prostate cancer | ||||
| Multiparametric MRI | Ga-68 PSMA-11 PET/MRI | |||
| Raw stringent approach | Alternative neighboring approach | Raw stringent approach | Alternative neighboring approach | |
| Tumor-positive regions detected/total | 174 | 327/475 | 275/412 | 383/520 |
| Sensitivity | 42% | 50% | 67% | 74% |
| p-value | < 0.001* | < 0.001* | ||
| Tumor-negative regions detected /total | 475 | 435/485 | 389/548 | 389/440 |
| Specificity | 79% | 90% | 71% | 88% |
| p-value | < 0.001* | 0.99** | ||
** Not statistically significant
Hicks and colleagues cited several study limitations, which included its retrospective approach and inclusion of subjects with a high risk if prostate cancer.


















