Addressing a question that has traditionally received little attention, researchers from South Carolina found that coronary CT angiography (CCTA) can accurately decide whether symptomatic patients at high risk of coronary artery disease actually need revascularization.
Researchers examined 185 symptomatic patients with a positive myocardial perfusion exam to evaluate CT's ability to determine the need for intervention, and if it's needed, which type. Among patients who had undergone both SPECT myocardial perfusion studies and conventional catheter angiography, CCTA showed more than 95% accuracy for determining the need for intervention, with no false negatives and just seven cases in which CT overcalled.
The findings could help address the persistent overuse of catheter angiography as a diagnostic exam, according to a presentation by Dr. U. Joseph Schoepf, from the Medical University of South Carolina, at the recent International Symposium on Multidetector-Row CT.
"There is no point in arguing about the relative accuracy of CCTA," Schoepf said. "What we should do now is take it into the clinical realm and test the efficiency of the test for clinical decision-making."
The goal of any test is to establish the best strategy for any individual patient, not an aggregate of patients, Schoepf said. But so far there is limited information about the role of CT in guiding patient management beyond the simple task of detecting and excluding significant stenosis. That's aggravated by the fact that the majority of cath exams performed are merely diagnostic and not followed by intervention.
CT is less invasive and less risky than catheter angiography, and if it can make the intervention decision in these high-risk patients, then other tests can potentially be avoided, Schoepf said. Thus, the study aimed to assess the efficacy of CT for differentiating patients with and without the need for revascularization and also for selecting the appropriate revascularization procedure.
The researchers specifically selected patients who had a high risk of coronary vascular disease -- somewhat against current guidelines that call for CCTA use only in low- and intermediate-risk patients, Schoepf said.
The 185 symptomatic patients (121 male, 64 female; mean age, 59 ± 10 years) had positive results at myocardial perfusion SPECT (summed stress score ≥ 9), and most were recruited from the Ralph Johnson Veterans Affairs Medical Center in Charleston. Exclusion criteria included a known history of coronary disease, indications for emergent catheterization, or contraindications to CCTA.
Revascularization: Yes or no?
The scan protocol depended on heart rate, rhythm, and body mass index. Conventional retrospective gating was used for 67 patients, with a mean estimated effective dose of 10.3 ± 4.1 mSv. Prospective electrocardiogram (ECG) triggering was used in 104 patients, with a mean estimated effective dose of 6.1 ± 2.9 mSv. Prospective, ECG-triggered, high-pitch spiral acquisitions were performed in 14 patients, with a mean estimated effective dose of 2.1 ± 1.3 mSv.
A radiologist and a cardiologist evaluated the CCTA data in consensus. They used a segment-based analysis based on the American Heart Association's (AHA) 15-segment model to determine the presence or absence of 50% or greater stenosis, adhering to the guideline that "only those lesions that have an effect on myocardial perfusion should be intervened on," Schoepf said.
Because the cohort had already undergone both nuclear stress exams and CCTA, those tests could be used to determine whether or not patients needed intervention, without knowledge of catheter angiography results. The resulting decisions were compared with the eventual strategy chosen by the combination of catheter angiography and SPECT.
"We considered whether revascularization was appropriate according to [AHA] guidelines: a match between a potentially flow-limiting lesion on CCTA versus a perfusion defect on the nuclear study," he said. "The coronary catheter angiography studies those patients underwent were evaluated in the same manner, where we also looked for matched lesions that had a nuclear myocardial perfusion defect."
The choice between percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) was based on the extent of vessel involvement, lesion complexity, medical factors, and so on.
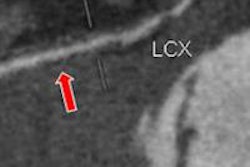
 Results in 185 symptomatic patients at high risk for coronary artery disease show that CCTA is highly accurate for identifying obstructive coronary disease and for selecting patients who need revascularization. For predicting the need for revascularization, CCTA demonstrated 100% sensitivity and 100% negative predictive value, with reasonable specificity and positive predictive values. All images courtesy of Dr. U. Joseph Schoepf.
Results in 185 symptomatic patients at high risk for coronary artery disease show that CCTA is highly accurate for identifying obstructive coronary disease and for selecting patients who need revascularization. For predicting the need for revascularization, CCTA demonstrated 100% sensitivity and 100% negative predictive value, with reasonable specificity and positive predictive values. All images courtesy of Dr. U. Joseph Schoepf.
High risk, but less disease than expected
The results showed no coronary artery disease in 42 patients (23%), nonobstructive disease in 68 (36%), left main disease in four (2%), one-vessel disease in 38 (21%), two-vessel disease in 14 (8%), and three-vessel disease in 19 (10%).
Even in this high-risk group, 23% of patients had completely normal coronary arteries, and another 36% had nonsignificant stenosis, Schoepf said. Put these two figures together, and in 59% of patients catheter angiography was arguably inconsequential, and patients did not benefit other than from ruling out disease.
The results are no outlier, mirroring almost exactly the results of a widely cited study by Dr. Manesh Patel and colleagues on the low yield of catheter angiography (New England Journal of Medicine, March 11, 2010, Vol. 362:10, pp. 886-895).
In an interesting wrinkle to the study, 12% of patients, or 23, had a negative calcium score and no atherosclerosis at all, despite being symptomatic and positive on nuclear perfusion. Thirty-one patients needed CABG according to conventional catheter angiography and other parameters, and all were identified by CCTA, Schoepf said. Based on CT, 48 appeared to need a stent; 41 received them. Three patients had critical obstructive disease, but all were in very distal segments not considered amenable to intervention.
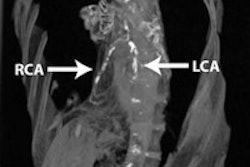
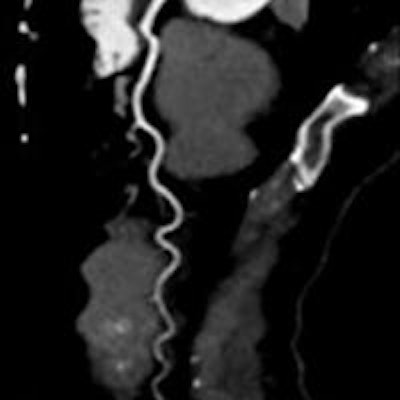
 In a 54-year-old man with suspected coronary artery disease, SPECT shows an abnormality in the apex (above), but CCTA (below) shows the coronary arteries are clear.
In a 54-year-old man with suspected coronary artery disease, SPECT shows an abnormality in the apex (above), but CCTA (below) shows the coronary arteries are clear.
"In patients with a high likelihood of coronary artery disease, CT is an effective gatekeeper for clarifying abnormal nuclear studies; similar decisions are made by CT for identifying patients with or without the need for revascularization compared to traditional catheter angiography," Schoepf concluded. CT missed no patients who needed revascularization, yielding only seven false positives. CT also makes decisions similar to catheterization for selecting PCI versus CABG, he added.
"That, of course, serves the goal of reducing the overwhelmingly high number of invasive diagnostic procedures that are still performed in this country and elsewhere," he said.