Postmortem CT can be an invaluable autopsy planning tool. With the help of a life-sized, 3D-enabled touchscreen table, pathologists can also view and manipulate images in 3D modes to locate pathology, perform virtual dissections, and decide on the best autopsy approach.
Medical autopsy is an important tool in determining cause of death, as postmortem examination does not always reflect the ground truth. Nonforensic postmortem imaging facilitates autopsy planning by offering a variety of complementary information prior to dissection, including localization of subtle or tiny lesions and bony abnormalities, as well as detection of air inside the body cavity.
A life-sized, 3D-enabled touchscreen table can be utilized to review postmortem CT images, enabling easy manipulation in multiplanar-reformation and volume-rendered modes and assisting with lesion localization and decisions about autopsy approach.
Back to the future
Postmortem imaging in medicolegal cases dates back to the earliest days of x-ray imaging. In 1896 -- within one year of its discovery -- x-ray was used to detect a bullet in a woman's skull. Its noninvasive nature and low cost, the ability to save virtual autopsy images, and its high data-acquisition speed make postmortem imaging a promising and complimentary way of acquiring data, even in nonforensic cases.
Unlike conventional autopsy that dissects the body, postmortem imaging maintains the integrity of the body while acquiring data; moreover, some studies have shown that postmortem imaging is less expensive than conventional autopsy, a noteworthy advantage in cases where the insurance company does not cover autopsy expenses. In addition, scheduling and performing postmortem imaging can be done in minutes, while an autopsy requires prior scheduling and takes hours to perform.
Data acquired through imaging can also be archived and accessed later at any time. Furthermore, postmortem imaging can play a very important role when autopsy is undesirable due to cultural or religious constraints. Other notable benefits include the ability to manipulate image data and provide permanent documentation.
Postmortem CT is currently being successfully utilized in some centers around the world to determine the cause of death. Studies have reported that the rate of "undetermined cause of death" dropped from 65% to 35% by implementing postmortem CT. In addition, postmortem CT scans can be very helpful for pathologists in planning autopsy procedures.
Postmortem images provide insight into the human body, which helps the autopsy team detect air within the body cavity; look for tiny lesions in areas hard to reach, such as bones; localize the lesions; and eventually plan the autopsy approach.
MGH project
In an ongoing project at Massachusetts General Hospital (MGH), we are performing whole-body CT scans as soon as possible after the patient's death. With support from an RSNA education grant, my colleagues and I have already performed more than 200 postmortem CT imaging studies under the guidance of Dr. Mannudeep Kalra and Dr. Sarabjeet Singh.
The cadavers undergo CT examination within an average of six hours from death and a range of two to 24 hours. As concern about radiation risk is lessened, human cadavers are scanned at multiple radiation dose levels to understand the effects of dose on CT image quality. The cadaver's arms are kept in a position so as not to cause artifact in the thorax, while the head is placed in a head rest to reduce beam-hardening artifact caused by skull bone.
After the exam, CT images are transferred from the scanner to a life-sized touchscreen table (Anatomage, San Jose, CA) for display. This life-sized table is 3D-enabled, which allows manipulation of imaging data in multiplanar-reformation and volume-rendered modes.
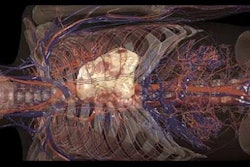
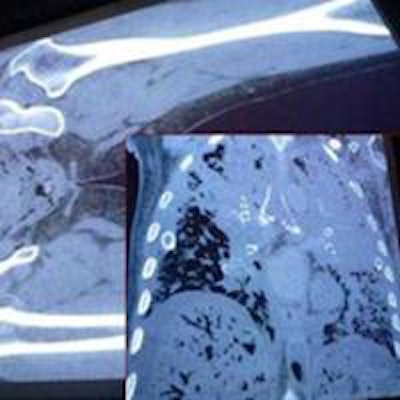
 Single-click multiplanar and volume-rendered images help in the evaluation of bony deformities and findings. All images courtesy of Dr. Sarvenaz Pourjabbar.
Single-click multiplanar and volume-rendered images help in the evaluation of bony deformities and findings. All images courtesy of Dr. Sarvenaz Pourjabbar.Postmortem whole-body images are presented to the autopsy team members so they can visualize a 3D model of the case with lines, tubes, and instruments inside the body; find the visible abnormalities; and cut through the virtual body to localize the findings.
 Postmortem imaging allows tubes and lines as well as internal instruments to be located prior to autopsy.
Postmortem imaging allows tubes and lines as well as internal instruments to be located prior to autopsy.Although the findings of postmortem CT images are conveyed in a written report to the pathology team, radiologists are also physically present to interact with pathologists and point out lesions on the images to help provide better understanding of anatomical localization.
Education
Postmortem imaging can also be valuable in medical education. Postmortem CT images acquired from cadavers allow medical students to virtually dissect through the layers of the human body, without fear of destroying human tissue. This library of cases could be used again and again, without the need for fresh cadavers for every batch. We at MGH have already initiated a collaborative project with Harvard Medical School students for learning anatomy and radiology-pathology correlation.
The few limitations of postmortem CT include limited availability of scanners to perform postmortem scans and a lack of contrast, which renders visualization of a few organs as suboptimal. However, postmortem imaging research is catching up with this limitation, as several studies have shown successful contrast administration with modified heart-lung machines.
 Postmortem air inside the body can be detected prior to dissection.
Postmortem air inside the body can be detected prior to dissection.Interpretation of postmortem images requires training to differentiate normal postmortem changes from premortem pathologies. Potential CT findings can be obscured by normal postmortem body changes such as brain swelling, gas formation, and lung edema, so it's important to scan as close to the time of death as possible.
 Postmortem CT images show cerebral hemorrhage, hemorrhagic metastasis, and intracranial hemorrhage.
Postmortem CT images show cerebral hemorrhage, hemorrhagic metastasis, and intracranial hemorrhage.Normal postmortem findings that should be considered when reporting CT findings include the following: loss of differentiation between gray and white matter, brain edema and swelling, putrefaction (gas formation), sedimentation of blood cells, clot formation in the heart and great vessels, and collapsed lungs.
 Normal postmortem findings include red blood cell sedimentation in the heart (1), gas formation (2), clot in the heart (3), and lung changes (4).
Normal postmortem findings include red blood cell sedimentation in the heart (1), gas formation (2), clot in the heart (3), and lung changes (4).In conclusion, whole-body CT imaging on a life-sized touchscreen table with 3D imaging capabilities can help pathologists detect and localize tiny or unavailable lesions so that the autopsy can be planned before it is performed. Detection of air inside the vessels and tiny bone lesions are findings that may be missed in conventional autopsy. Virtual dissection with touchscreens allows easy manipulation of imaging data, which helps in localization and autopsy approach.
Dr. Sarvenaz Pourjabbar is a research fellow in radiology at Massachusetts General Hospital in Boston.