Giant cell arteritis
Clinical:
Giant cell arteritis (GCA) or temporal arteritis is the most common vasculitis
of large and medium sized areteries [1].
It is
characterized by granulomatous infiltrates
in the
wall of large and medium-sized arteries [2]. Extracranial
GCA most frequently involves the aortic arch and subclavian
and axillary arteries [1]. Affected
patients are
almost exclusively over the age of 50 years (the prevalence rises with
increasing age) [1,2] and female [2]. The
disease is
also more common among whites, compared to other racial groups [3] and
the highest reported rates are in Scandinavia and North America [4].
The disease primarily affects the extracranial carotid branches and the aorta (aortic involvement is found in 15% of GCA patients and it is the most common form of aortitis in North America accounting for 75% of cases [3]), and rarely the central pulmonary arteries [1]. Classic symptoms of GCA include tender and swollen temporal arteries, temporal headache, jaw claudication, and vision loss [1]. Systemic symptoms include fatigue, weight loss, low-grade fever, polymalgia rheumatica, athralgia, and tenosynovitis can be found alone or in combination in more than 50% of affected patients [1].
Aortic GCA typically remains asymptomatic during the early phase, but results in late complications such as aneurysms and dissections [1]. Patients with aortic GCA are 17 times more likely to develop thoracic aortic aneurysms compared to the general population [1].
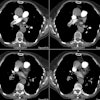
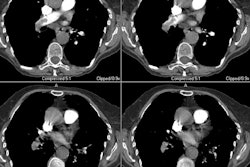
X-ray:
There is evidence of arterial wall thickening (greater than 1.5 mm), stenosis, annuloaortic ecatsi,a or aneurysm formation [1,2,3]. Lesions are long, segmented, and tapered at both ends [2].
PET imaging will demonstrate abnormal tracer uptake in the aortic arch or large thoracic arteries in more than half of affected patients [3].
REFERENCES:
(1) Radiographics 2010; Castaner E, et al. When to suspect pulmonary vasculitis: radiologic and clinical clues. 30: 33-53
(2) AJR 2010; Spira D, et al. Imaging of primary and secondary inflammatory diseases involving medium-sized vesels and their potential mimics: a multitechnique approach. 194: 848-856
(3) Radiographics 2011; Restrepo
CS, et al. Aortitis: iimng
spectrum of the infectious nd inflammatory
conditions
of the aorta. 31: 433-451
(4) Radiographics 2011; James OG, et al. Utility of FDG PET/CT in inflammatory cardiovascular disease. 31: 1271-1286