Pseudocoarctation:
Clinical:
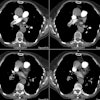
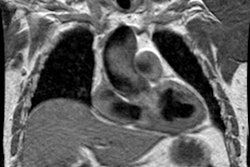
Pseudocoarctation is due to a rare "kinking" or buckling of the aortic arch at the ligamentum arteriosus in which the first portion of the descending aorta is elongated, somewhat dilated, and sharply deviated (anteriorly). There is no pressure gradient across the buckled segment, no stenosis, and no collateral circulation [3]. The condition has also been defined as an anatomical narrowing or stenosis of the thoracic aorta in the region of the ligamentum arteriosum, with little or no impediment to blood flow [2]. It is usually seen in middle aged men with hypertension, although decreased lower extremity pulses are not observed. The condition is associated with an increased incidence of congenital heart disease particularly bicuspid aortic valve, VSD, PDA, and coexistent true coarctation. Management is conservative therapy as long as the patient remains asymptomatic and aortography fails to demonstrate aneurysmal dilatation beyond the aortic deformity [2].X-ray:
Affected children may demonstrate a high, chimney shaped arch. In adults, radiographic findings are similar to those seen with true aortic coarctation. The contour of the arch is typically larger than normal- appearing as a rounded mass in the upper left mediastinum- with an abrupt indentation at its inferior margin. A second rounded shadow having a superior convexity is seen more inferiorly and represents an end-on view of the descending aorta. Rib notching has NOT been reported in association with pseudocoarctation. Angiography will reveal the tortuous high rising aorta with buckling of the distal arch and the absence of a significant pressure gradient across the area of narrowing. Even in the absence of a pressure gradient, post-stenotic dilation may occur due to loss of laminar flow with turbulence stressing the integrity of the aorta just distal to the narrowed area (laminar flow can be lost when the aortic lumen is decreased to 78% of it's original cross-sectional area) [2]. No collateral vessels should be identified.REFERENCES:
(1) J Thorac Imaging 1994; Munjal AK, et al.
Magnetic resonance imaging of pseudocoarctation of the aorta: A case report.
9: 88-91
(2) Vascular Surgery 1972; Prian GW, et al. Pseudocoarctation: Diagnosis, etiology, natural history with emphysis on timing and technique of surgical correction. 6(4): 198-209 (No abstract available)
(3) J Cardiovasc Comput Tomogr 2011; Bolen MA, et al. Pseudocoarctation of the aorta and crossed fused ectopic kidney assessed by multidetector computed tomography. 4: 405-406