Coal Miners Pneumoconiosis:
Clinical:
This disorder is due to coal dust inhalation and the inhaled carbon
is the offending agent (not silica). As coal particles are inhaled,
they are predominantly deposited in the respiratory bronchioles because
of slow flow in these airways [3]. In the lower portions of the lung,
these particles are cleared more rapidly because of better lymphatic
flow [3]. The particles that are not cleared by lymphatic flow, are
taken up by alveolar or interstitial macrophages (macrophages are not
destroyed upon carbon ingestion) [3]. At this stage the process is
termed anthracosis (and this can also be seen in smokers and
urdan-dwelling individuals) [3]. The "coal macule" is the histologic
lesion and represents the carbon-containing macrophages surrounded by a
network of collagen fibers and fibroblasts (initially it measures 1-2mm
in diameter) [3]. The macules accumulate in the upper lobes,
particularly around respiratory bronchioles [3]. As the disease
progresses, the nodules coalesce and eventually grow into progressive
massive fibrosis [3].
Many of these patients may have a mixed disease (ie: concurrent silicosis) due to heavy exposure to silica in coal mines. The disorder generally requires a period of at least 10 years exposure and it is radiographically indistinguishable from silicosis. The disease extent directly relates to the amount of exposure and the disease does not progress once exposure has been stopped. Many of these patients have a mixed disease, however, due to concurrent silica exposure. As with silicosis, the risk for tuberculosis is increased in patients with coal workers pneumoconiosis [2]. Types of disease include:
1- Simple form: Characterized by small nodular opacities (2-5mm) with an upper lobe predominance, which less commonly calcify than in silicosis. Pulmonary function tests remain within normal limits and the disorder is arrested upon discontinuation of exposure.
2- Complicated form: Characterized by large opacities/nodules (>1cm) which are radiographically indistinguishable from the conglomerate masses of silicosis. This complicated form is also referred to as "progressive massive fibrosis" and emphysematous changes. FEV1, FVC, and diffusing capacity are all decreased.
3- Caplan's Syndrome: This syndrome is characterized by rheumatoid arthritis with pulmonary rheumatic nodules in coal workers (Caplan syndrome occurs in 0.75-1.5% of patients with pneumoconioses [3]). The nodules typically measure between 0.5 to 5 cm in size and may cavitate. Patients are rheumatoid factor (+). The nodules often develop concomitantly with joint disease, but they may precede the onset of arthritis by months or years.
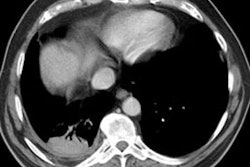
X-ray:
Computed tomography: On CXR, there are small round nodular opacities and occasionally reticular or reticulaonodular opacities [2]. The nodules are usually 1-5 mm in size and tend to be less well defined compared to those found in silicosis [2]. Calcification of the nodules is seen in 10-20% of patients on CXR- often as a central dot [2]. On CT, small nodules are seen diffusely throughout the lungs, but with an upper lung zone predominance [2]. Calcification of the nodules is found in 30% of patients [2]. Lymph node enlargement is seen in 30% of patients [2]. Egg-shell calcification is uncommon (only 1.3% of patients) [2]. In addition, centrilobular emphysematous changes are common in patients with CWP.
Progressive massive fibrosis with development of conglomerate masses
is seen in complicated CWP [2].
The nodules associated with coal workers pneumoconiosis are positive
on FDG PET imaging [3].
REFERENCES:
(1) Radiol Clin North Am 1991 Sep;29(5):931-941
(2) Radiographics 2006; Chong S, et al. Pneumoconiosis: comparison
of imaging and pathologic findings. 26: 59-77
(3) Radiographics 2012; Shah SH, et al. AIRP best cases in
radiologic-pathologic correlation. Coal workers pneumoconiosis. 32:
2047-2052