CHICAGO - Taking a high-quality portable chest x-ray can be difficult, leading to an overexposed image when digital radiography equipment is used. One solution to reduce overexposures is a new data-mining tool, according to a Tuesday presentation at the RSNA 2011 meeting.
Bedside chest radiography, whether using analog or digital equipment, presents challenges. Variations in tube-to-detector distance, grid alignment, patient motion, and the size of a patient can all affect image quality. With computed radiography (CR) or digital (DR) radiography equipment, the temptation to overexpose an image exists because the dynamic range of digital detectors and image processing capability can compensate for a poor image.
While the radiology department at the University of Chicago Medical Center had a quality assurance program in place that identified overexposed images, along with regular training reviews for radiologic technologists, it did not reduce the number of motion-degraded and overexposed portable chest exams.
A Web-based data-mining tool combined with a continuous quality improvement initiative has radically changed this unwanted status quo. The department wrote its own software program that extracts the exposure values from its CR system (Fujifilm Medical Systems USA) for each bedside chest radiograph. Specifically, the sensitivity (S) value, a numeric approximation of the radiation dose to the imaging plate, is extracted from the exam's DICOM header.
The tool also extracts the medical record number of the patient, the accession number, the study date and time, and the name of the technologist who performed the exam. The department defined an overexposed chest radiograph as having an S-value of less than 150.
The radiology department began using the data-mining tool on November 1, 2010. Dr. Neel Patel, a third-year radiology resident, explained that a trial run of the software took place during the first 30 days; however, it worked so well that the data acquired were incorporated into the formal evaluation period, which ended February 18. Data were collected for the aggregate daily baseline overexposure rate of bedside chest radiographs, and also were calculated for each of the approximately 50 technologists who performed the exams.
Technologists were then ranked based on the cumulative number of overexposed exams. Five technologists with the greatest proportion of overexposed exams were identified for individualized training and feedback. They received individual one-on-one training over the next four weeks. Team leaders reviewed bedside chest radiograph technique and technical factors affecting radiation exposure during the individual meetings.
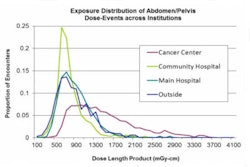
"Data are displayed in an interactive graphical format that shows the range of exposures for all cases during a selected period," Patel explained. "The format is easy to use. When mouse-clicked, individual segments of the graph reveal the identities of the technologists who performed a study or studies, and provide the details of each individual examination."
Great emphasis was placed on not criticizing the technologists for their results. "The approach was constructive, and it was individual," Patel noted.
"In a large group session, instructional points and feedback are given at a general level, and technologists apparently did not relate this to what they were doing," he said. "Group training does not provide enough personal incentive and empowerment to change behavior."
The efficiency of the automated data-mining tool combined with individualized training has positively affected the department. Prior to its implementation, 1,726 (18.1%) of 9,525 portable chest exams performed between November 1, 2010, and February 18, 2011, were overexposed. Between March 13 and July 31, the aggregate overexposure rate decreased to 12.2%.
Individual performance also improved among the technologists with the highest overexposure rankings. The technologist with the most overexposures dropped from a 51% rate to a 28% rate. Another technologist's overexposure rate decreased by 50%, reaching 18% during the postintervention period. The other three had changes of 2% to 3%.
"The chest section of the department is satisfied with current levels of improvement," Patel said. "With time, we will be able to assess the sustainability of the current model of teaching and feedback."
Patel did not discuss what would occur if a technologist did not improve his or her performance after the training intervention. To date, no punitive actions have been taken.