Patients experience less discomfort during optical colonoscopy than they do with virtual, according to a study from the University of California, Los Angeles. It's the pain that lingers after conventional colonoscopy that tips the patient-preference balance toward VC, the research team concluded.
"The majority of patients who require colon screening nowadays are not undergoing colon screening, and one of the hopes of VC is to increase patient compliance and increase the number of patients being screened," said Dr. David Lu from the UCLA department of radiology at the International Symposium on Virtual Colonoscopy in Boston in October. "But several studies comparing patient acceptance issues between CTC and colonoscopy have been conflicting. Some show a preference for VC, some a preference for colonoscopy."
In efforts to develop a screening exam that could attract hesitant patients to screening, there is a trend in virtual colonoscopy these days to offer, or at least investigate, minimal-prep VC protocols, which would presumably include some combination of fecal tagging, electronic cleansing or stool subtraction, and computer-aided detection to ensure adequate sensitivity in the cluttered reading environment.
The UCLA researchers screened 19 patients of mixed risk for colorectal cancer in their prospective study, first with virtual colonoscopy, then with conventional colonoscopy no later than three weeks after the initial exam.
Patient surveys were given before each test for expected preferences, and then after the tests, "they were asked to repeat the survey based on ... what their experience really was (more than) two days after each test," Lu said. "They were asked to rate procedure on a five-point scale for inconvenience, hunger levels, how palatable was the prep, and for the actual procedure itself, the discomfort during and after the procedure, and also the duration of discomfort after procedure."
VC bowel preparation consisted only of 30 cc of a 40% barium sulfate solution (Tagitol V, E-Z-EM, Lake Success, NY) with each meal for three days prior to scanning; there were no other dietary restrictions until the last day before the exam. On that day, the subjects were restricted to the contents of a prepared low-fiber meal kit (NutraPrep, E-Z-EM) along with the barium.
Following automated CO2 insufflation of the colon (PROTOCO2L, E-Z-EM), low-dose abdominal CT was performed on a 16-slice scanner at 50 mAs, 100 kVp, 1-mm collimation, and 0.5-mm reconstruction interval. An attending GI radiologist evaluated the images with primary 2D and 3D problem-solving software, but no computer-aided detection (CAD) or electronic cleansing software.
Four patients dropped out after VC, leaving 15 to undergo both exams.
"We think that some of these patients signed up for the study just to get the VC for free," Lu said. "But regardless, we ended up with 15 patients who could be evaluated for survey responses, but 19 patients that could be evaluated for technical quality."
The 15 remaining patients underwent conventional colonoscopy following a double-dose phosphosoda prep, he said.
The results of the pre-exam survey showed that 15/15 patients preferred the virtual colonoscopy prep over the conventional kind. After the exam, 14/15 preferred the virtual colonoscopy prep with regard to inconvenience, discomfort, hunger levels, and anxiety. The VC prep was widely preferred; only embarrassment levels showed no statistically significant difference between the two exams.
 |
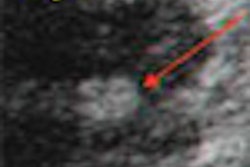
| All images courtesy of Dr. David Lu. |
Compared to optical colonoscopy as the gold standard, however, VC had two false-negative adenomas larger than 10 mm. One was a flat lesion, and none were high-grade dysplasia. Three false-positives were seen in two patients with severe sigmoid diverticulosis due to small untagged fecal balls, recognized for their low density.
"We know that for those patients that had incomplete fecal tagging in the distal part of the colon, pretty much it was all because they ... identified as being constipated," Lu said. "In terms of evaluating these images, we really didn't see any beam-hardening artifact from the barium that compromised the evaluation, to our surprise," he said. Otherwise, fecal tagging was generally adequate.
In the postexam survey, patients actually reported greater discomfort for minimal-prep VC compared to conventional colonoscopy -- not surprising, Lu said, because all of the colonoscopy patients received conscious sedation.
 |
"But here's the key -- the discomfort level after and the discomfort duration after the exam was much less for (VC) versus optical colonoscopy," he said. "For optical colonoscopy you can see that on average, patients had discomfort that lasted more than two hours. So that was the most important factor contributing to why the overall (VC) procedure was (perceived as) much better."
 |
Larger cohorts will be needed to confirm the preliminary results. Certainly, patients who have known constipation or diverticulosis should be excluded from minimal-prep VC, Lu said. Finally, he said, the accuracy of minimal-prep VC will benefit from the application of CAD and electronic cleansing.
By Eric Barnes
AuntMinnie.com staff writer
February 23, 2005
Related Reading
Iodine tagging regimen yields best VC results, January 17, 2005
Laxative-free VC appears promising, November 10, 2004
VC antispasmodics show mixed distension results, real patient-acceptance gains, August 27, 2004
Reduced-prep VC with tagging works after failed colonoscopy, March 7, 2004
In virtual colonoscopy, nothing beats a good prep, July 16, 2002
Copyright © 2005 AuntMinnie.com