SAN FRANCISCO - A decade into worldwide dose reduction efforts, most community hospitals and imaging centers still haven't adopted low-dose CT techniques, according to a study presented on Thursday at the 2012 Society for Pediatric Radiology (SPR) meeting.
Pediatric dose reduction at these facilities still lags behind that of academic centers, and the use of advanced dose reduction techniques, such as iterative reconstruction, is even rarer. This has resulted in higher radiation exposure levels at community-based facilities compared to academic centers, concluded a comprehensive radiation exposure assessment from Oregon Health and Science University (OHSU).
Since the first study appeared 10 years ago linking CT radiation with higher long-term cancer risk, an international initiative has been under way to reduce imaging doses in children, including the 2008 launch of the Image Gently campaign, said OHSU's Dr. Kristopher Spinning in his talk.
Children's hospitals in particular -- including OHSU's -- have made radiation reduction a priority, Spinning said, with measures ranging from increased scrutiny of CT requests to implementation of low-dose CT protocols and technical advances. Dose reductions resulting from these efforts have been documented at children's hospitals, he said.
"However, most pediatric CT scans are done outside of children's hospitals, at adult-focused community hospitals," where adoption of low-dose techniques has not been evaluated, Spinning said. The OHSU study aimed to compare size-specific dose estimates at the hospital with those of multiple adult-focused community hospitals in the region from 2010 and 2011.
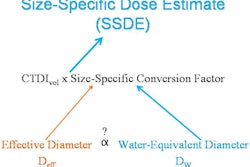
Spinning, along with colleagues including David Patterson and Dianna Bardo, compared the doses using size-specific dose estimates (SSDEs), a new method that allows factoring due to patient size. The results were compared among OHSU, whose reference dose levels are comparable to those of the largest SSDE study to date, and community imaging settings in four states, grouped as follows:
- Group A included 250 patients who underwent weight-based CT protocols at OHSU without automatic exposure control (AEC) and filtered back projection (FBP) reconstruction.
- Group B, representing a kind of future target for dose reduction, included 216 patients undergoing 60% CT dose index volume (CTDIvol)-reduced scans reconstructed with a blend of iterative reconstruction (IR) and FBP.
- Group X included 164 pediatric CT scans acquired at 39 community imaging centers in four different states. These scans were acquired using a variety of scan techniques, predominantly AEC, and traditional FBP, Spinning said.
Data collected included patient age, lateral dimension as determined on the scout image, scan type, CTDIvol, reference phantom diameter, and the name of the facility, he said. Statistical analysis of the results used regression models to analyze differences in SSDE by group, while controlling for potential confounding variables.
Radiation dose levels by reconstruction method and facility type
|
"The mean SSDE between group A and X, as well as between group B and X, showed statistically significant differences," Spinning said, with group A demonstrating a mean SSDE of 11.0, Group B a mean SSDE of 4.4, and Group X a mean SSDE of 17.2.
Radiation dose by demographic and technical factors
|
||||||||||||||||||||||||||||
The statistical significance of the differences persisted when scans were broken out by body region: chest, abdomen/pelvis, and chest/abdomen/pelvis, Spinning said.
The mean SSDE for matched scans in community chest, abdomen/pelvis, and chest/abdomen/pelvis scans was 1.7, 1.3, and 1.6 times higher than the mean SSDE for matched scans in Group A (p < 0.0001). The value was 5.0, 2.8, and 3.7 times higher than the mean SSDE for matched scans in Group B (p < 0.0001).
In dose distribution, there was overlap between Group A and the community imaging centers; however, the outliers in Group X ranged from 12 to 29 times higher than the mean SSDE in groups A and B, he said.
"Regional community hospitals and imaging centers have not uniformly adopted the low-dose CT practices, although there is considerable overlap between groups A and X," Spinning concluded. "More community outreach and education are needed to encourage implementation of low-dose protocols outside the children's hospitals. Looking toward the future, technical advances such as iterative reconstruction can provide a means to achieve even greater SSDE reduction than is possible with filtered back projection alone."
The adoption of iterative reconstruction technology should be encouraged at all imaging centers, he said.