Recent studies indicate that CT scanning with an adaptive statistical iterative reconstruction (ASIR) algorithm offers better image quality at a lower radiation dose. But a new algorithm, called model-based iterative reconstruction (MBIR), could be even better than ASIR, according to a presentation today at the International Society for Computed Tomography (ISCT) meeting in San Francisco.
In two Tuesday morning presentations, investigators from a consortium of U.S. universities detailed their work on the algorithm, which was developed over nearly a decade by GE Healthcare of Chalfont St. Giles, U.K., which also developed ASIR. Researchers claim that MBIR outperforms previous efforts to maximize the utility of low-dose CT exams, with researchers reporting excellent image quality and enhanced lesion conspicuity.
Still, MBIR does have some drawbacks. Image processing times are extremely slow, first and foremost. More than an hour is needed to process a typical 600-slice dataset, researchers evaluating the algorithm told AuntMinnie.com.
But processing speed will be resolved in the commercial version, says GE, which is working with the research consortium to speed MBIR's development. The technique is the result of more than eight years of research at Notre Dame University in South Bend, IN; Purdue University in West Lafayette, IN; and the University of Michigan in Ann Arbor, according to GE.
 |
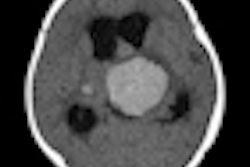
| Filtered back projection (above) and MBIR (below) reconstructed from the same raw dataset and the following acquisition parameters: 120 kVp, 75 mAs, and 64 x 0.625 mm. Note the small low-attenuation mass in the right adrenal gland on the MBIR image (arrow). All images courtesy of Dr. Rendon Nelson. |
 |
The company makes no claims about the work-in-progress technique and has set no target date for its commercialization. But physicists and radiologists working with MBIR are enthusiastic about its clinical potential to deliver sharper images with less radiation.
Duke University School of Medicine professor of radiology Dr. Rendon Nelson, who leads a consortium of radiologists evaluating the algorithm, gives it high marks compared to other commonly used image-processing techniques. In an interview with AuntMinnie.com, Nelson outlined the differences between filtered back projection (FPB), ASIR, and MBIR.
In the beginning, there was filtered back projection, which was developed in the 1970s by U.K.-based EMI (of Beatles fame) for the first CT scanners. The technique remains a fast, robust method for image processing, he said, but it leaves a lot of the raw image data out of the picture.
"To a certain extent it's like looking at something in the dark," Nelson said. "FPB makes a lot of assumptions about the x-ray beam: It assumes the beam is perfect at the level of the voxel, that it's a focal spot on the x-ray tube as a point source, that it's a perfect voxel at the level of the patient and the detector -- although none of those conditions exist. That's why [FPB] basically leave a lot of information untapped: noise information and information about adjacent voxels."
"For FBP we pretty much ignored the size of the focal spot, and the same thing for the CT detectors," said Jiang Hsieh, Ph.D., chief scientist for GE Healthcare. That's not optimal considering that the submillimeter spatial resolution of a state-of-the-art CT scanner constitutes a larger percentage of the 1 x 1-mm detector size, Hsieh said.
A step up from filtered back projection is GE's ASIR, a simple model-based reconstruction algorithm that performs some algebraic computations to compare image data to a noise model, Nelson said.
Guessing high and low
The term "iterative" refers to a kind of computerized guessing game in which the algorithm predicts the correct noise and attenuation information, learns if it's too high or too low, and then tries again, gradually approaching the truth and adjusting the image as a result, Nelson said. But the iterations can only work so well because they are limited to a single noise model.
Unlike FBP, ASIR "still assumes that the x-ray beam is perfect, but it looks more at the statistics of the beam rather than just making all of the assumptions," Nelson said. "It goes back and forth from the slice data to the raw data until it comes up with an image that approximates the model."
The MBIR algorithm works a lot harder, performing multiple iterations from multiple models. It analyzes the x-ray beam from the focal spot, then analyzes the shape of the beam as it passes through the patient three-dimensionally, and again once more as the beam strikes the x-ray detector on the other side of the patient.
"So the focal spot, the patient, and the detector are all modeled three-dimensionally with multiple iterations," Nelson said. "And in doing so you get a lot more information."
The more complex MBIR algorithm models two parts of the CT system: system optics or geometry, as well as system statistics such as image noise, Hsieh explained.
"There are two components in noise: one is photon flux -- typically, when I have less photons, the noise in the signal is higher than if I had very high photons," Hsieh said.
 |
| Unlike filtered back projection reconstruction (above), which relies on assumptions about the x-ray beam, MBIR (below) analyzes the beam at three points: at the focal spot, as it passes through the patient's body, and, finally, at the level of the x-ray detector. |
 |
Modeling and removing predictable noise
The second noise component comes from the scanner itself. "There's a lot of electronics in a CT system," Hsieh said. Scanners "convert x-ray photons into light photons, then using a photodiode, convert that into an electrical signal," he said. The photodiode introduces noise and the digitization process introduces noise. [With MBIR] "we tried to model all of the noise sources in a CT system," he said.
In layman's terms, the difference between FBP and ASIR is like the difference between a black and white and a color TV, Nelson said.
"The resolution is no better, the sound is no better, the brightness is no better -- it just goes from being black and white to color," he said. "So it's an improvement, but not as big an improvement as the next step, MBIR, which would be analogous to going from an analog color TV to a digital LED TV that's much sharper, much brighter, has a blacker background, a higher frame rate, and better sound quality."
A slow go
In the research version of MBIR currently available to investigators, the computation-heavy algorithm takes a lot of computer time, and image reconstruction is slow. For example, using a typical 600-slice CT dataset, FBP reconstruction might take a minute or two, ASIR might require three to four minutes, and MBIR might need an hour and a half.
"That's the bad news," Nelson said. "The good news is that the image quality is a lot better and there's a lot less noise." He added that he's confident computation times will drop substantially as high-speed computers equipped with parallel processors get even faster. And developers have already cut MBIR's processing time of 70 hours for the typical dataset down to the current one to two hours.
"Remember that CT scanners in the 1970s took 45 minutes to an hour to get a slice," Nelson said.
"As we look to bring this to market, we're working with IBM and Intel on the most advanced processor capabilities," said Daniel Morris, GE's CT marketing chief. "So the experience with the prototype is not what the performance will be."
Slow processing simply means that very time-sensitive or emergent CT applications are out of the picture for now, leaving plenty of potential for other promising low-dose applications such as oncology, Nelson said.
How low a dose?
Just how low will radiation dose be with MBIR reconstruction?
"Based on phantom and preliminary patient data, we think we can maybe go down to about a 75% reduction in dose and get the image quality we're getting now with 100% filtered back projection," Nelson said. At 75% or so dose reduction, an abdominal image acquired at 200-225 mAs might reasonably be obtained at 75 mAs with equivalent image quality. "So it has the potential to dramatically change the way we do things," Nelson said.
Just as with ASIR images, the reduced-dose MBIR images have a "waxy" appearance that does not detract from their diagnostic quality. "It's something that everyone who reads these will have to get used to," Nelson said.
Still, the diagnostic quality of MBIR images has not been fully studied, as assessments are based not on formal studies but on preliminary results from phantom studies and on image and diagnostic quality assessments from the dozen or so radiologists participating in the research consortium, Nelson said.
The consortium of radiologists at 10 to 12 U.S. centers functions as "way to try to get a lot of information about new technology in short period of time," Nelson said. Sample images are sent for diagnosis, image-quality questionnaires are completed, and the group meets once a year to discuss the results.
Meanwhile, GE is embarking on an international multicenter trial to evaluate the efficacy of low-dose imaging with ASIR. Right now the consortium is working on developing imaging protocols for the study, Morris said, and patient recruitment is slated to begin later this year.
"Radiation is an issue now, and I think sometimes it keeps us from doing the right thing for the patients," Nelson said. "What I'm really hoping is that radiation will become less of an issue so that we can use CT more effectively to make the correct diagnosis. MBIR is a good technique that makes such a contribution to patient care."
By Eric Barnes
AuntMinnie.com staff writer
May 18, 2010
Related Reading
Filtering software boosts CT image quality, lowers dose, May 7, 2010
Reduced dose can still yield acceptable pediatric CT images, April 22, 2010
Automated exposure control delivers uneven CT dose reduction, April 15, 2010
CT doses, widely variable in Europe, are reduced by staff efforts, March 6, 2010
ASIR cuts dose in Crohn's disease patients, December 4, 2009
Copyright © 2010 AuntMinnie.com