In the midst of a large multicenter trial on virtual colonoscopy, radiologists from U.S. military hospitals reported in this month's American Journal of Roentgenology that colorectal lesions are easier to detect with the aid of 3-D primary interpretation of CT virtual colonoscopy data rather than 2-D, especially when electronic bowel cleansing and stool-tagging techniques are also employed.
What is more, the group told AuntMinnie.com in a follow-up e-mail that it had completed its trial of 1,233 average-risk patients, and found that the hybrid virtual colonoscopy technique was even more sensitive than conventional colonoscopy for detecting polyps 8 mm and larger. The still-unpublished results could potentially spur a new wave of interest in widespread virtual colonoscopy screening.
Still, the researchers cautioned in their report that their hybrid technique tends to introduce a number of errors that can lead to false positives unless they are reviewed and eliminated in a conventional 2-D imaging environment.
"For our ongoing multicenter screening trial in average-risk patients, we have found that polyp conspicuity is greatly increased using the 3-D endoluminal perspective," wrote Dr. Perry Pickhardt and Dr. Jong-Ho Richard Choi in September's American Journal of Roentgenology. "Although less sensitive for initial detection, the complementary 2-D images improve specificity and are therefore indispensable for distinguishing true polyps from a variety of pseudopolyps seen on 3-D imaging" (AJR, September 2003, Vol. 181:3, pp. 799-805).
The types of 3-D pseudopolyps the group encountered are well known to virtual colonoscopy providers: residual fecal debris, impacted diverticula, extrinsic compression, and the ileocecal valve, according to the team, which is from Walter Reed Army Medical Center in Washington, DC, and F. Edward Hébert School of Medicine in Bethesda, MD. The use of electronic cleansing and fecal tagging also improves the diagnostic abilities of virtual colonoscopy, the group added, but these techniques introduce even more equivocal findings and false positives into the mix.
Virtual colonoscopy technique
Before undergoing virtual and optical colonoscopy on the same day, patients have a standard purgative bowel prep with phosphosoda (Fleet 1 preparation, Fleet Pharmaceuticals, Lynchburg, VA), also consuming 500 mL of 2.1% of Scan C, a barium contrast material (Lafayette Pharmaceuticals, Lafayette, IN), as well as diatrizoate meglumine and diatrizoate sodium as laxatives. Patients administer their own room-air bowel insufflation to tolerance.
CT images are acquired with a four- or eight-detector LightSpeed or LightSpeed Ultra CT scanner (GE Medical Systems, Waukesha, WI) with collimation set at 1.25 to 2.5 mm, table speed increment at 13.5 mm to 15 mm/sec., 100 mAs, and 120 kVp.
The V3D virtual colonoscopy system (Viatronix, Stony Brook, NY) is used to generate volume-rendered 3-D images, enabling virtual fly-throughs (video link for high-speed connections only) of the colon along an automated lumen centerline. A mouse click enables easy navigation between 2-D and 3-D images, according to the authors.
Electronic cleansing
"Although originally intended to reduce or eliminate the need for colon purgation, electronic cleansing is also of benefit in the prepared colon," Pickhardt and Choi wrote. "Removing opacified residual fluid digitally allows 3-D evaluation of colonic mucosa that would have otherwise been obscured," enabling the detection of neoplasia submerged in fluid. The picture is not perfect, however. Rather than clearly depicting the submerged mucosa, the linear artifact where air-fluid level interfaces with the colon wall "has been likened to residue that remains in (a) tub after (a) bath," they wrote.
 |
| Electronic cleansing of contrast-opacified luminal fluid on 3-D virtual colonoscopy in an asymptomatic 65-year-old man undergoing colorectal cancer screening. Uncleansed (left) and cleansed (right) images from the same endoluminal perspective show increase in visualized mucosal surface after digital subtraction of residual fluid. Characteristic linear artifact where air-fluid level interfaces with colon wall (arrows, right) has been likened to residue that remains in a tub after a bath. Images and caption used with permission of the American Roentgen Ray Society from AJR, © September 2003, Vol. 181:3, pp. 799-805. |
The authors prefer water-soluble iodinated contrast material for opacification of fluid, and a diluted barium solution for tagging particulate debris. And despite the technical advances, the combination of prone and supine imaging is still needed to ensure adequate evaluation of the entire colonic mucosa, they stated.
As it stands, electronic cleansing is an important aid in finding polyps submerged in fluid; the major problem is that the process creates 3-D artifacts that mimic true polyps.
"Incomplete cleansing due to suboptimal opacification of luminal fluid can result in bizarre artifacts that may have the appearance of polyposis," they wrote. "The geographic planar distribution of these abnormalities generally prevents them from being confused with true abnormalities. Although these artifacts can be distracting initially, they are easily ignored with experience."
Untagged or poorly tagged fecal material lying dependently in a luminal fluid pool is another source of pseudopolyps related to electronic cleansing, according to the authors, but these tend to be mobile and can thus be differentiated from true polyps by comparing prone and supine data of the same region. Still, they take extra time to evaluate and exclude, and represent the negative side of a tradeoff of 3-D, compared with the advantage of increased conspicuity of submerged lesions.
 |
| Electronic cleansing artifact seen on 3-D virtual colonoscopy resulting from suboptimal fluid opacification in a 62-year-old man undergoing screening. Cleansed (left) and uncleansed (arrows, right) axial images show 2-D correlate of cleansing artifact, with jagged appearance at air-fluid level on subtracted image. (Images and caption used with permission of the American Roentgen Ray Society from AJR, © September 2003, Vol. 181:3, pp. 799-805.) |
Polypoid artifacts related to partial-volume effects are a more serious shortcoming of the primary 3-D read, according to the group. Such artifacts tend to occur where air-fluid levels interface with the colon wall, especially when a meniscus effect is also present, the group wrote. Air-fluid haustral-fold interfaces are another characteristic location of polypoid artifacts, making evaluation of the uncleansed 2-D images vital for accurate interpretation. Since these artifacts result from the cleansing process, they are often present on the electronically cleansed 2-D images as well.
"Last of all, trapped air bubbles in an otherwise fluid-filled lumen can also give rise to convincing pseudopolyps on 3-D images," they wrote. "In such cases, the uncleansed 2-D images yield a rapid explanation."
 |
| Above, pseudopolyp due to partial-volume effect at air-fluid wall interface in average-risk 54-year-old man undergoing virtual colonoscopy screening. Three-dimensional endoluminal image obtained with electronic cleansing shows 6-mm sessile lesion. (Images and caption used with permission of the American Roentgen Ray Society from AJR, © September 2003, Vol. 181:3, pp. 799-805. |
 |
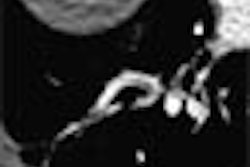
| Above, uncleansed 2-D image of the same average-risk 54-year-old man undergoing VC screening obtained with patient in supine position shows air-fluid-wall interface (arrow) corresponding to level of "polyp" on cleansed 2-D images (not shown). Note the utility of uncleansed images in avoiding a false-positive finding. (Image and caption used with permission of the American Roentgen Ray Society from AJR, © September 2003, Vol. 181:3, pp. 799-805.) |
Barium tagging
The authors believe that barium tagging is very useful even in the prepared colon, noting that adherent stool represents the most important cause of false positives in VC. Moreover, the heterogeneous appearance of stool masquerading as a polypoid lesion can be helpful in distinguishing it from true polyps, but the presence of identifiable air in the fecal material is rare.
"These lesions will often appear polypoid on the 3-D endoluminal image, but the dense nature is apparent on the 2-D images with soft-tissue window settings. This increased attenuation could be overlooked on 2-D images with the wider window setting that is typically used for polyp detection."
The group is currently investigating the translucency feature of the V3D system as another solution.
"Recent technical advances have paved the way for using 3-D endoluminal rendering for primary polyp detection in CT colonography," the group concluded. "Solid-stool tagging and electronic cleansing of opacified fluid are useful diagnostic adjuncts to colon purgation. In addition to the advantages, however, diagnostic pitfalls associated with these techniques must be recognized to maintain an acceptable level of specificity."
In an e-mail to AuntMinnie.com, Pickhardt said that over the course of the study he has become a strong proponent of primary 3-D reading.
"We have completed our multicenter screening trial (1,233 patients) and I have already submitted it for publication (no word yet)," Pickhardt wrote in the e-mail. "Without going into specifics, our results are very encouraging for screening VC using a primary 3-D approach. VC compared favorably with the ‘gold standard’ (optical colonoscopy) -- in fact, VC was actually slightly more sensitive than optical colonoscopy for detecting adenomas 8 mm and greater (which we were able to show by 'segmentally unblinding' VC findings to the endoscopists)."
Virtual colonoscopy's sensitivity, specificity, and accuracy were all above 90% at the 8-mm threshold, despite the low prevalence of disease (i.e., adenomatous polyps), he wrote, adding that the results could generate new interest in widespread VC screening, though with a few important caveats.
- The trial's "hybrid" approach differed significantly from that of most earlier VC studies, most importantly in its use of primary 3-D reading, which Pickhardt believes was the main factor behind the improved results compared to previous results in a low-prevalence population, for example in a recent Mayo Clinic study, and in a Medical University of South Carolina study.
- The use of electronic cleansing and stool tagging have also been rare in published studies, he said.
- Segmental unblinding turned many would-be VC false positives into optical colonoscopy false negatives.
- The use of multidetector-row CT and thin collimation may have also improved the results somewhat.
In a paper to be published in the December 2003 American Journal of Roentgenology, the group directly compares the 3-D capabilities of three different virtual colonoscopy systems, according to Pickhardt. "The differences are staggering and help explain why most investigators aren't using a primary 3-D approach," he wrote. "Their systems simply aren't designed to do it!"
By Eric BarnesAuntMinnie.com staff writer
September 2, 2003
Related Reading
Virtual colonoscopy: 2-D vs. 3-D primary read, June 3, 2002
Copyright © 2002 AuntMinnie.com