While penile fracture is rare, it's a serious and painful urologic condition for which surgery is typically advised. According to an article in the September issue of RadioGraphics, MRI's excellent tissue contrast and multiplanar capabilities make it the presurgery planning tool of choice.
According to the authors, MRI can easily demonstrate the extent and location of injuries, and help determine whether surgery is warranted (Radiographics, Sept. 2000, Vol.20:5. pp.1397-1405).
Penile fracture is caused by an external force that tears the thinned tunica albuginea of the erect penis, or less commonly, the corpus spongiosum or urethra. It can occur during intercourse, nonphysiologic manipulation, rolling over in bed with an erection, or by direct injury to the penis.
The integrity of the tunica albuginea and the absence or presence of urethral injury are the two most important factors determining the need for surgical intervention, according to Drs. Moon-Hae Choi, Bohyun Kim, and colleagues from the departments of radiology and urology at Samsung Medical Center in Seoul, South Korea.
The tunica albuginea is a fibrous sheath that surrounds each of the three parallel masses of erectile tissue in the body of the penis: two lateral corpora cavernosa and the ventromedial corpos spongiosum. The erectile bodies are composed of venous spaces called sinusoids that are distended with blood during erection. The Buck fascia is a fibrous sheath that surrounds the three erectile masses together and the corpos spongiosom separately. The distal portion of the corpos spongiosum forms the glans of the penis.
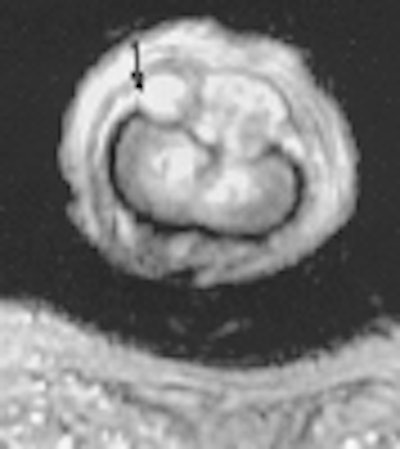
Figure 1 (165KB)
Figure 2 (187KB)
Figure 3 (165KB)
The tunica albuginea thins from about 2 mm to 0.5 - 0.25 mm during erection, making it vulnerable to injury. Surgical repair is generally recommended for patients with suspected tear of the tunica albuginea. Urgent surgical intervention is needed in the case of urethral or spongiosal involvement due to a higher complication rate, according to the authors.
At the same time, other conditions such as intracavernosal or extratunical hematoma can be treated conservatively. While surgery is not always essential for penile fractures, it can prevent complications such as fibrous plaque formation and angulation, and reduce the time of convalescence, they wrote.
In part because severe pain or swelling in suspected tears often precludes thorough physical examination, several radiologic methods have been used to image suspected tears. Among them, cavernosography can be useful for identifying suspected corpus cavernosal tears, but it is invasive and carries potential complications, according to the authors. Ultrasound has also been used effectively to evaluate penile trauma, and in a study appearing in the British Journal of Urology, researchers found the exact site of a tear in the tunica albuginea in 6 of 7 patients (1993, Vol.72, pp. 228-229).
"However, despite being readily available and easy to perform, US does not always allow diagnosis of a tunical tear and often cannot be used due to severe pain and swelling of the injured penis," the RadioGraphics authors wrote. At the same time, MRI's excellent tissue contrast and multiplanar capabilities have made it a useful diagnostic tool for the evaluation of penile fracture.
"Because the tunica albuginea is well demonstrated as a low-signal-intensity structure at both T1- and T2-weighted MR imaging, this modality is best suited for the evaluation of the integrity of the tunica albuginea even in patients with severe pain and swelling of the penis," they wrote.
The study evaluated 9 patients who presented between 1995 and 1998 with suspected penile fracture. All of the patients, aged 29-54, underwent MR imaging. Trauma had occurred in all cases during vaginal intercourse, and most patients presented with acute, painful swelling of the penis, the authors wrote.
Methods
Patients underwent MR imaging with a pelvic phased-array coil. Doctors obtained axial T1-weighted spin-echo images and axial, coronal and sagittal T2-weighted fast spin echo images. In some cases, additional T1-weighted axial and sagittal images were obtained following administration of intravenous gadolinium contrast. Adequate support and correct positioning under the surface coil was essential for good-quality images, the authors wrote.
Results
As confirmed at surgery, tear of the tunica albuginea was correctly diagnosed with MR in 7 of 9 patients. The tears were clearly visualized as discontinuities of the low-signal-intensity tunica albuginea. While the remaining two patients had intact tunica albuginea, MRI diagnosed intracavernosal hematoma in one, and extratunical hematoma in the other. These two patients did not undergo surgery.
"In our series, MR findings concerning the size, location, and orientation of tunical tear were confirmed at surgery," the authors wrote. "The tears were located in the ventral portion of the corpus cavernosum in 6 patients, and in the lateral portion in the remaining patient."
The experience with contrast is inconclusive and needs further study, Dr. Bohyun Kim wrote in correspondence with AuntMinnie.com.
"Contrast seems to be helpful in demonstrating the tunical tear or surrounding hematoma in selected cases, but overall accuracy in demonstrating the integrity was comparable between T2-weighted imaging and gadolinium-enhanced T1-weighted imaging," he wrote.
MR imaging is an excellent technique for evaluating the integrity of the tunica albicans in patients with acute penile trauma, the authors concluded.
"Not only can it demonstrate the integrity of the tunica albuginea and the extent and location of tears, it can assess injury to the corpus spongiosum and urethra ... MR imaging can be very helpful in decision-making."
By Eric BarnesAuntMinnie.com staff writer
September 25, 2000
Let AuntMinnie.com know what you think about this story.
Copyright © 2000 AuntMinnie.com



















