Researchers are highlighting a new non-invasive imaging tool that can create real-time, 3D images and maps using MRI of contractions during labor, their results being published March 14 in Nature Communications.
A team led by Hui Wang, PhD, from Washington University in St. Louis, reported success with this method, called electromyometrial imaging, and noted that it could help with labor management strategies.
"This study ... demonstrates that electromyometrial imaging can noninvasively provide rich information on human uterine activation patterns," Wang and colleagues wrote.
Nearly one in three women deliver via cesarean, most of which are performed when labor arrests. But cesareans increase the risk of maternal morbidity and neonatal respiratory morbidity compared to vaginal delivery. Preterm birth also puts infants at risk, and it occurs in more than 10% of births around the world.
These risk factors make accurate assessment and interpretation of uterine contractions important for diagnosing labor dysfunction and preterm labor. In their study, Wang and colleagues proposed a new way to map out and provide a timeline for measuring contractions through electromyometrial imaging.
How does the method work? It integrates fast anatomical MRI to acquire uterine images with a multi-channel, surface scanning electromyogram, the latter of which uses sensors placed along the woman's belly to measure contractions during labor.
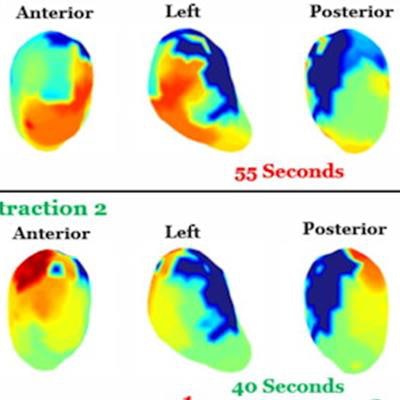
In Wang and colleagues' research, women wore up to 24 MRI patches containing up to 192 MRI-compatible fiducial markers around the body surface. From there, the data were combined and processed into 3D uterine maps, with warm colors indicating areas of the uterus activated earlier in a contraction and cool colors showing areas activated later. Gray areas indicate inactive regions of the uterus.
The technique creates a sequence of maps that shows a visual timelapse of contractions. The timelapse shows where contractions start, how they spread, and potential patterns one might expect from a typical pregnancy compared to a complicated one.
 In this example, two adjacent contractions were imaged during labor. Electromyometrial imaging shows that the first contraction starts from the middle segment of the uterus and propagates up and down simultaneously. The entire electrical activation underlying the contraction takes around 55 seconds. The second contraction starts from the fundus region (top of uterus) and propagates down in a faster (40 seconds) and synchronized manner than the first contraction. Image and caption courtesy of Washington University in St. Louis, MO.
In this example, two adjacent contractions were imaged during labor. Electromyometrial imaging shows that the first contraction starts from the middle segment of the uterus and propagates up and down simultaneously. The entire electrical activation underlying the contraction takes around 55 seconds. The second contraction starts from the fundus region (top of uterus) and propagates down in a faster (40 seconds) and synchronized manner than the first contraction. Image and caption courtesy of Washington University in St. Louis, MO.Wong and colleagues tested the method on 10 pregnant women, five of whom were becoming first-time mothers (nulliparous) and five of whom will have borne multiple children (multiparous). The team reported successful mapping of the contractions and wrote that based on the morphology of the uterine surface from electromyometrial imaging with high spatial resolution, the inactivated myometrium regions could be well-delineated.
"Based on our findings in both nulliparous and multiparous subjects, the entire uterus is not active during uterine contractions, especially in the early phase of the labor," the team wrote.
The study findings show that there are no consistent early activation regions in different uterine contractions and that long-distance propagation of activation is also not evident in human uterine contraction, the authors noted.
In nulliparous women, electromyometrial imaging showed "weaker, less synchronized, and less fundus-dominated contractions" at the early stage of active labor; contractions became much stronger and synchronized in the later stage of active labor, the researchers wrote.
For multiparous women, imaging showed stronger uterine contractions, represented by larger values for contraction activation curve slopes, fundal early activation ratios, and a higher percentage of myometrium activated during a contraction. These findings suggest that multiparous women experience faster maturation of contractions compared to their nulliparous counterparts.
The study results could help clinicians develop a "normal term atlas" consisting of electrical recordings that cover the entire labor process, according to the authors. This kind of "map" could be used in clinical trials that would test interventions to prevent complications such as labor arrest, preterm birth, and postpartum hemorrhage, the authors wrote.



















