French researchers have developed a new high-resolution cardiac MRI technique that can diagnose myocardial injuries in patients with COVID-19, according to a study published September 18 in the European Journal of Radiology.
Also, the method is faster than conventional cardiac MRI methods, detects more heart defects, and doesn't require repeated breath holds -- a significant difficulty for COVID-19 patients, according to the authors.
"In patients with history of COVID-19 infection associated with troponin rise, the method allows for detailed characterization of myocardial injuries in acceptable scan times and without the need for repeated breath holds," wrote first authors Aurelien Bustin, PhD, and Dr. Soumaya Sridi of the University of Bordeaux.
In cardiac MRI, late gadolinium enhancement (LGE) is a standard tool widely used for diagnosing various myocardial diseases, primarily by detecting injured areas in the heart muscle. LGE can diagnose heart attacks, for instance.
High-resolution (HR) late gadolinium enhancement techniques have been developed that provide good contrast between injured and healthy myocardial tissue, but they require repeated breath holds by patients and are hampered by prolonged acquisition times, according to the authors. Moreover, the increasing need for cardiac MRI during the COVID-19 pandemic is requiring more efficiency in clinical workflows, and accelerated techniques are critically needed, the authors wrote.
To meet these challenges, the University of Bordeaux team aimed to introduce an accelerated free-breathing isotropic HR-LGE technique for the diagnosis of COVID-related myocardial injuries.
First, the researchers developed an undersampled navigator-gated HR-LGE (acquired resolution of 1.25 mm3) sequence combined with advanced patch-based low-rank reconstruction. They tested the sequence in a resolution phantom and then validated the approach in 23 patients with structural heart disease.
Next, they enrolled 20 patients in the acute phase of COVID-19 at the University of Bordeaux hospital between May and November 2020. The patients had laboratory-confirmed COVID-19 infection associated with troponin rise. Imaging was performed on a 1.5-tesla scanner (Magnetom Aera, Siemens Healthineers) with a dedicated 32-channel spine coil and an 18-channel body coil.
Two patients had histories of healed myocardial infarction and 18 had no history of cardiac disease. All patients had been hospitalized, including 11 in an intensive care unit, with five requiring mechanical ventilation.
The researchers analyzed image sharpness, quality, signal intensity differences, as well as the diagnostic value of free-breathing HR-LGE compared against conventional breath-held low-resolution LGE.
In all patients (n = 43), including those in the validation study, the technique allowed for acquisition times of 7 minutes and 21 seconds at 1.25 mm3 resolution, compared with an average of approximately 16 minutes at 1.4 mm3 isotropic resolution on low-resolution late gadolinium enhancement (LR-LGE), the researchers found. Compared with LR-LGE, HR-LGE also showed higher image quality and comparable signal intensity differences.
In patients with structural heart disease, all LGE-positive segments on LR-LGE were also detected on HR-LGE (80/391) with 21 additional enhanced segments visible only on HR-LGE (101/391).
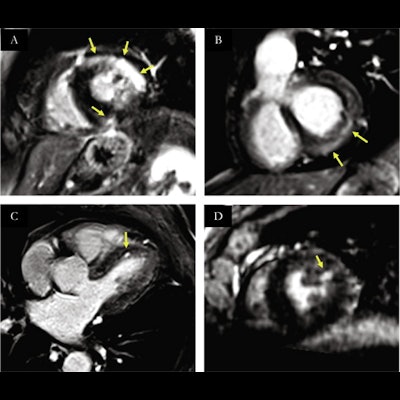
 Spectrum of myocardial injuries on reformatted free-breathing high-resolution LGE after COVID-19 infection. Yellow arrows indicate areas with LGE. (A) intramural and subepicardial LGE on the anteriolateral and inferoseptal segments, consistent with myocarditis. (B) subepicardial LGE on inferobasal and infero-latero-basal segments, consistent with myocarditis. (C) focal subendocardial LGE on antero-septal segment consistent with micro-infarction. (D) focal subendocardial LGE on anterolateral segment consistent with microinfarction. Image courtesy of the European Journal of Radiology.
Spectrum of myocardial injuries on reformatted free-breathing high-resolution LGE after COVID-19 infection. Yellow arrows indicate areas with LGE. (A) intramural and subepicardial LGE on the anteriolateral and inferoseptal segments, consistent with myocarditis. (B) subepicardial LGE on inferobasal and infero-latero-basal segments, consistent with myocarditis. (C) focal subendocardial LGE on antero-septal segment consistent with micro-infarction. (D) focal subendocardial LGE on anterolateral segment consistent with microinfarction. Image courtesy of the European Journal of Radiology.Overall, a definite diagnosis using the new sequence was obtained in 15 out of 20 of the COVID-19 patients, including myocarditis in nine, multiple microinfarctions in two, myocardial infarction in two, and takotsubo cardiomyopathy in two.
"Undersampled free-breathing isotropic HR-LGE can detect additional areas of late enhancement as compared to conventional breath-held LR-LGE," the authors wrote.
The researchers noted what they described as a rather alarming observation -- that most of the studied patients did not present with cardiac-specific clinical symptoms. This suggests the need for systematic troponin tests during the acute phase of COVID-19 infection, and for a broader use of HR-LGE cardiac MRI in patients with a history of COVID-19 infection, the authors stated.
"There is a critical and urgent need to assess the prevalence of silent scars in the population infected by COVID-19, in order to better appreciate the cardiac risk that the pandemic may weigh on the global population in the near future," they concluded.