Atherosclerosis progresses undetected and is known as the silent killer. But cardiac CT can identify early signs of the disease in healthy people -- an important new finding for developing strategies to prevent it, according to studies published September 20 in the journals Circulation and Heart.
In both studies, the researchers highlighted the limits of current diagnostic measures for identifying the disease, namely CT coronary artery calcium (CAC) scores. CAC scores are the current clinical standard for identifying patients at risk, as they measure the hardened plaque that accumulates in arteries, a hallmark sign for atherosclerosis.
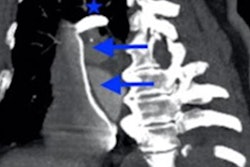
In the study in Circulation, a group of Swedish researchers found the use of coronary CT angiography (CCTA) detected levels of atherosclerosis in 42.1% of patients, despite the fact that some had CAC scores of 0.
"A zero CAC score does not exclude adults from having atherosclerosis," said lead author Dr. Göran Bergström, PhD, of the University of Gothenburg's Institute of Medicine in Gothenburg, Sweden, in a news release from the American Heart Association (AHA).
Bergström and colleagues analyzed data from 25,182 Swedish adults between the ages of 50 and 64 with no history of a prior heart attack or cardiac intervention. The patients underwent both CAC scans and coronary CT angiography scans between 2013 and 2018.
The researchers found that the prevalence of CCTA-detected atherosclerosis increased with increasing CAC scores. Among those with a CAC score greater than 400, all had atherosclerosis and 45.7% had significant stenosis.
In patients with CAC scores of 0, however, 5.5% had atherosclerosis and 0.4% had significant stenosis. In participants with CAC scores of 0 and intermediate 10-year risk of atherosclerotic cardiovascular disease, 9.2% had atherosclerosis that was verified on CCTA scans.
Prevalence estimates had excellent external validity and changed marginally when adjusted to the age-matched Swedish background population, the study authors added.
"Measuring the amount of calcification is important, yet it does not give information about noncalcified atherosclerosis, which also increases heart attack risk," Bergström said.
The CAC paradox
In the study in Heart, the researchers addressed whether the progression of coronary artery calcium is associated with different levels of physical activity in healthy individuals. They discovered a paradox: There was a positive association between physical activity and the prevalence and progression of hardened coronary plaque, regardless of baseline CAC scores.
"In this large prospective study of apparently healthy men and women, physical activity was associated with a higher prevalence of CAC at baseline and with a faster progression of CAC over follow-up," wrote first author Dr. Ki-Chul Sung, PhD, of Sungkyunkwan University School of Medicine in Seoul, Korea.
In a large cohort from two South Korean hospitals, the study authors analyzed CT CAC scores from 25,485 subjects as well as their physical activity over a median duration of three years. Physical activity was graded by the investigators as inactive, moderately active, or health-enhancing physically active, which was equivalent to running 6.5 km a day.
Sung and colleagues found the group performing the higher medically recommended levels of physical activity had the highest baseline burden of advanced calcified plaque.
Estimated average baseline CAC scores in participants who were inactive, moderately active, and highly active were 9.5, 10.2, and 12, respectively. Compared with participants who were inactive, the estimated adjusted five-year average increases in CAC in moderately active and highly active participants were 3.2 and 8.2.
In addition, higher physical activity was associated with faster progression of CAC scores both in participants with a CAC score of 0 at baseline and in those with prevalent CAC, the researchers added.
"Our findings should not be interpreted as a harmful effect of physical activity, but, rather, need to be taken into account when evaluating the progression of CAC in patients who exercise to reduce cardiovascular risk," Sung and colleagues concluded.
In an accompanying editorial, Dr. Gaurav Gulsin, of the University of Leicester in England, and Dr. Alastair Moss, of the University of British Columbia, Canada, wrote that the CAC paradox suggested in the Heart study should not result in paradoxical care for patients.
"This study fuels a wider discussion of some of the key limitations regarding the use of the coronary artery calcium scan to monitor coronary artery disease progression," they wrote.
"While proponents would argue that it is an effective tool to screen for subclinical atherosclerosis in asymptomatic individuals, clinicians should be cautious regarding the overuse of this test in otherwise healthy individuals," they concluded.