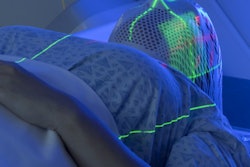
A change in one major health insurer's utilization management policy led to a significant increase in shorter, hypofractionated radiotherapy treatments for women with breast cancer -- in agreement with evidence-based treatment guidelines, according to the findings of a study published on April 16 in JAMA Oncology.
In 2016, the insurer changed its utilization management policy for radiation therapy for women with early-stage breast cancer. The payor decided to no longer reimburse conventional fractionalized radiotherapy for women if they were eligible for hypofractionated treatments. Exceptions could be made only for certain situations and after consulting with payor representatives.
The change led to a significant increase in hypofractionated radiotherapy for women subject to the policy as well as their peers who shared the same doctors.
"The utilization management policy was associated with increased rates of hypofractionated radiotherapy use, even when accounting for a secular trend of increasing hypofractionated radiotherapy use in the general population," wrote the authors, led by Dr. Ravi Parikh from the University of Pennsylvania Perelman School of Medicine.
A three- to five-week course of hypofractionated radiotherapy is a cost-effective and convenient alternative to traditional fractionated radiation treatments, the authors noted. While the American Society for Radiation Oncology (ASTRO) has recommended the shorter approach for at least some patients with breast cancer for almost 10 years, as few as one-third of eligible women choose to participate in hypofractionated treatments.
So when a major insurer created a utilization management policy in favor of hypofractionated radiotherapy for women with early-stage breast cancer, the researchers saw an opportunity to study the policy's effects on women choosing to undergo the treatment.
For their study, Parikh et al used claims and enrollment data from 10,540 women with insurance through one of 14 common health plans. The women all had early-stage breast cancer and were eligible for hypofractionated radiotherapy based on the ASTRO guidelines.
The percentage of both fully insured and self-insured patients who elected to undergo hypofractionated radiotherapy skyrocketed during the course of the study period. In 2012, 22.4% of fully insured patients and 20.3% of self-insured patients chose hypofractionated treatments. By 2018, that percentage rose to 82.3% and 79.8% for fully insured and self-insured patients, respectively.
The increase in hypofractionated radiotherapy was significantly greater for patients subject to the new policy than for their self-insured peers. However, self-insured patients who visited clinicians treating patients subject to the policy were also more likely to undergo hypofractionated radiotherapy than self-insured patients not linked to clinicians treating patients subject to the policy.
"Utilization management in oncology may be associated with increases in evidence-based practice in populations that are both directly and not directly subject to the policy," the authors wrote.
Notably, the authors did not find a significant decrease in cost for patients who underwent hypofractionated radiotherapy compared with traditional treatments. This could be because of the relatively mild difference in hypofractionated treatments between patients subject to and not subject to the policy.
The authors also could not determine a causal relationship between the policy and treatment types, nor could they determine whether practice factors, such as practicing at an academic hospital, had an effect on the use of hypofractionated radiotherapy.
Nevertheless, the policy was associated with a direct and spillover effect on the evidence-based hypofractionated treatment of women with early-stage breast cancer.