PET/CT performed better than planar scintigraphy or SPECT for determining which patients with neuroendocrine tumors are most likely to benefit from peptide receptor radionuclide therapy (PRRT), in a study published in the September issue of the Journal of Nuclear Medicine.
Using a simple formula called a Krenning score, researchers found that PET/CT with a gallium-68 (Ga-68) DOTATATE radiotracer performed significantly better than planar scintigraphy and SPECT with an indium-111 (In-111) pentetreotide radiotracer, particularly when lesions were smaller than 2 cm (JNM, Vol. 60:9, pp. 1266-1269).
A Krenning score is a reproducible method designed to quantitatively estimate the expression of somatostatin receptor (SSTR) in patients with neuroendocrine tumors. Physicians traditionally have used In-111 pentetreotide scintigraphy or SPECT and Krenning scores to assess these patients, but little is known about the accuracy of PET/CT in determining lutetium-177 (Lu-177) DOTATATE PRRT eligibility.
"Our study aimed to compare the Krenning scores derived from the various imaging modalities and assess the impact on treatment decision-making," explained co-lead author Dr. Thomas Hope from the University of California, San Francisco (UCSF) in a statement.
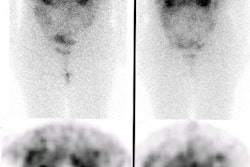
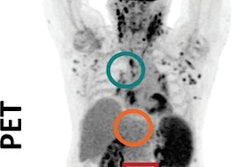
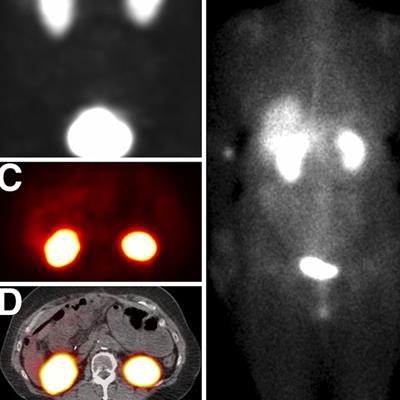
 SSTR PET reflects higher Krenning scores than In-111 pentetreotide in low-volume disease. The patient was graded as having a Krenning score of 4 on SSTR PET (A) but 0 on SPECT (B, C, and D) and planar imaging (E). MIP = maximum-intensity projection. Images courtesy of JNM.
SSTR PET reflects higher Krenning scores than In-111 pentetreotide in low-volume disease. The patient was graded as having a Krenning score of 4 on SSTR PET (A) but 0 on SPECT (B, C, and D) and planar imaging (E). MIP = maximum-intensity projection. Images courtesy of JNM.The retrospective study included 150 patients with suspicion or biochemical evidence of neuroendocrine tumors who underwent both Ga-68 DOTATATE PET/CT and In-111 pentetreotide imaging with planar scintigraphy and SPECT within one week. Three readers independently graded the images using the Krenning score based on the lesion with the highest uptake. The volume and extent of tumor burden, lesion size, and maximum standardized uptake value (SUVmax) were also compared with the Krenning scores.
"The higher the Krenning score, the higher the predicted uptake of the targeted therapy," Hope said.
The detection rate of SSTR-positive disease was the highest with Ga-68 DOTATATE PET/CT (72%), compared with In-111 pentetreotide planar imaging (23%) and SPECT (38%), and the difference was statistically significant. In addition, among patients with a Krenning score of at least 3, the detection rate of In-111 pentetreotide planar imaging (15%) and SPECT (24%) was much lower for lesions smaller than 2 cm than for larger lesions. Most patients with lesions smaller than 2 cm would not have qualified for PRRT based on In-111 pentetreotide imaging, but they would appear to be candidates based on Ga-68 DOTATATE PET/CT.
"This head-to-head comparison research study shows for the first time that Ga-68 DOTATATE PET/CT results in higher Krenning scores than In-111 pentetreotide imaging in determining eligibility for PRRT, especially for neuroendocrine tumor patients with lesions smaller than 2 cm," noted co-lead author Dr. Jeremie Calais from the University of California, Los Angeles (UCLA).
Patients should be aware, however, that even if there is a high Krenning score from Ga-68 DOTATATE PET/CT, it "does not always mean that Lu-177 DOTATATE PRRT is appropriate as the next treatment," Hope said. "There is a great amount of work left in order to understand how to use Ga-68 DOTATATE PET/CT to select patients for treatment moving forward."