A dual-phase angiography procedure based on conebeam CT (CBCT) principles that was used during transcatheter arterial chemoembolization (TACE) can predict treatment response in hepatocellular carcinoma (HCC) tumors long before MRI is traditionally applied at one-month follow-up, researchers wrote in Radiology.
In their study of 29 patients with HCC, the researchers from Johns Hopkins University showed a significant relationship between tumor enhancement at angiography-based CBCT right after TACE -- and MR imaging response a month later, suggesting that the CBCT technique can be used to predict response without waiting for follow-up.
"Early assessment of the effectiveness of TACE and monitoring of tumor response are paramount to the identification of treatment failure, guidance of future therapy, and determination of the interval for repeat treatment," wrote Dr. Romaric Loffroy and colleagues (Radiology, November 9, 2012).
Early assessment of TACE effectiveness and monitoring of tumor response are crucial for identifying failed procedures, guiding therapy, and determining the optimal interval for repeat treatments, the authors explained. MR and, far more rarely, CT are used to assess response one to three months after follow-up using the Response Evaluation Criteria in Solid Tumors (RECIST).
"However, assessment of anatomic response in the early post-treatment period can be misleading because the absence of a reduction in tumor size does not mean an absence of response and often does not correlate with the degree of tumor necrosis," the authors wrote. "Consequently, a reduction in tumor enhancement at imaging has been used more accurately as a biomarker of tumor response."
Imaging a month after the procedure with MR makes the results too late for intraprocedure modification, which is especially difficult when patients need repeat treatment, they wrote. Post-TACE imaging with doxorubicin-eluting beads can be done with CT or MRI a day after the procedure, but a procedure that could predict tumor response at the time of treatment would be even better inasmuch as tumor response has been shown to be an independent predictor of survival.
"Recently, C-arm CT has emerged as a new and widely used imaging technology in the angiography suite, enabling the acquisition of a 3D dataset generated from one rotational run with use of conebeam CT principles," they wrote.
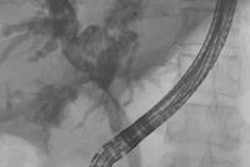
C-arm CT is enabling the acquisition of 3D datasets in a single rotation of the C-arm using CBCT, which can be used to examine tumor-feeding vessels and parenchymal stain during TACE procedures, Loffroy and colleagues explained. A new development allows two-phase images to be acquired with a single contrast injection with two sequential back-to-back acquisitions that show both arterial and venous phases rather than requiring two separate acquisitions and contrast injections.
 |
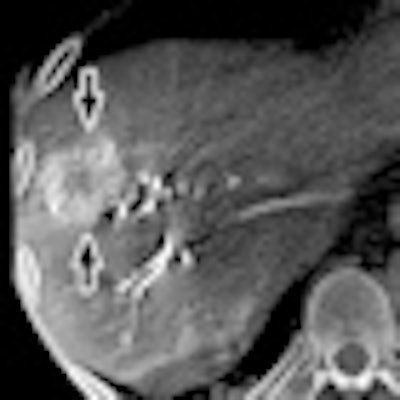
| Images show arterial- and venous-phase MRI and CBCT in a 58-year-old man with HCC in right lobe secondary to hepatitis C virus. MR images were acquired one month before and one month after TACE using doxorubicin-eluting beads; CBCT was acquired before and immediately after TACE. (A) Arterial-phase images obtained before TACE. MR image shows a 32-mm mass in right lobe with 75% enhancement. CBCT shows mass with similar enhancement (80%). (B) Venous-phase images obtained before TACE. MR image shows mass with partial washout (50% enhancement). CBCT shows mass with almost the same decrease in enhancement (65%). (C) Arterial-phase images obtained after TACE. MR image shows mass with almost no enhancement (5%); tumor size remains unchanged (31 mm). CBCT shows intraprocedural mass enhancement decreased by 100%, which allowed prediction of objective EASL response at one month. (D) Venous-phase images obtained after TACE. MR shows mass with almost no enhancement (5%). Conebeam CT scan shows intraprocedural mass enhancement decreased by 92%, which allowed prediction of an objective EASL response at one month. Images republished with permission of the RSNA from Loffroy et al, Radiology, November 9, 2012. |
The researchers aimed to determine whether the new technique could be applied intraoperatively to predict TACE response compared to MRI results at one-month follow-up. They analyzed 50 HCC lesions in 29 patients (16 men, 13 women; mean age, 61.9 ± 10.7 years) who had undergone TACE after injecting beads loaded with 100 mg of doxorubicin hydrochloride (25 mg/mL) and mixed with an equal amount of nonionic contrast.
All patients underwent the C-arm angiography-based CBCT technique (Allura Xper FD20, Philips Healthcare) before and immediately after TACE. This system was equipped with XperCT software that enabled CBCT-like acquisition and volumetric image reconstruction on a separate computer. The dual-phase conebeam CT prototype feature, not yet commercially available, enables the XperCT option to be modified to obtain two sequential, back-to-back conebeam CT scans encompassing both early arterial and delayed or venous phases in a single contrast injection, Loffroy and colleagues wrote.
CT tumor enhancement was evaluated retroactively by readers blinded to the MR results; two patients with unevaluable data at CBCT were excluded from analysis, leaving 27. The group used logistic regression models to compare tumor enhancement between modalities.
Correlation with MR at 1 month
One-month follow-up imaging with MR showed complete or partial tumor response in 74% of lesions on the arterial phase and 76% in the venous phase, the study team reported. Paired t-test analysis showed significant reduction in tumor enhancement in both modalities (p < 0.001).
The volume enhancement reductions correlated linearly with MR findings, with high estimated correlations for first (k = 0.89) and second (k = 0.82) phases. In addition, multilogistic regression showed a significant relationship between CBCT tumor enhancement after TACE and complete or partial tumor response at MR for arterial and venous phases. The radiation dose for dual-phase, as measured in a piglet model, was 3.08 mSv.
"Our results showed that intraprocedural dual-phase conebeam CT allowed monitoring and quantification of changes in tumor enhancement during TACE and assisted in accurate prediction of response to therapy," Loffroy and colleagues wrote.
Early assessment of treatment response is important -- especially in determining the need for repeat treatment, they wrote. Recent studies have demonstrated changes in vascular and cellular biomarkers including contrast enhancement and diffusion within hours after therapy, and these changes generally precede anatomic changes measured by RECIST guidelines. However, the optimum time for assessing TACE response remains unknown, with the results of two previous contrast-enhanced ultrasound studies favoring anywhere from two days to a week.
Previous studies couldn't address whether changes in tumor enhancement at TACE could be used to predict response via European Association for Study of the Liver (EASL) guidelines, which this study accomplished with the use of integrated angiography and CBCT, they said. Contrast enhancement is a reflection of cellular viability, where areas of tumor enhancement are considered viable and unenhanced regions reflect tissue necrosis.
"In comparison to other systems (angiography and MR units), our approach of using conebeam CT has the added advantage of being readily available in many practices internationally," they wrote. And although the use of dual-phase CBCT didn't increase prediction of tumor response by more than a single acquisition in the arterial phase, the technique demonstrates tumor-feeding vessels in the early arterial phase and enhancing parenchyma in the delayed venous phase.
The angiography-based dual-phase CBCT technique also gets by on one contrast injection rather than two using conventional techniques, saving contrast and reordering workflow to cut procedure time. The software allows simultaneous comparison of MR to CT or pretreatment to post-treatment images.
Study limitations included the small sample size, and the fact that all patients were undergoing their first TACE procedures, which typically yield better results than subsequent embolizations, the authors wrote.