
Top Story

Latest News


Sponsored
We care about what you think.
October 30, 2023


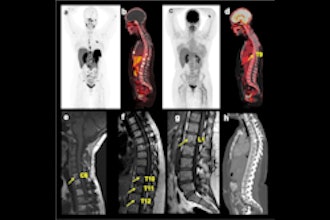
Cases of the Week
Check out our Cases of the Week!




More from AuntMinnie
FDA clears Philips Zenition 30 mobile C-arm
April 22, 2024


American Shared Hospital Services mourns passing of CEO
April 22, 2024

GE expands collaboration with Elekta via MIM subsidiary
April 22, 2024
Evergreen Theragnostics raises $26M
April 19, 2024

Segmed partners with Beacon Health System in Indiana
April 19, 2024




Accuray opens training facility in Switzerland
April 18, 2024

Lumicell's Lumisight, LumiSytem get FDA nods
April 18, 2024
