Imaging researchers have long known that chest tomosynthesis is more sensitive than conventional x-ray for detecting malignant pulmonary lesions, while producing lower radiation dose than CT. Now, they are zeroing in on a precise role for this unique technology.
Researchers from the University of Trieste in Italy used digital radiography (DR) tomosynthesis as part of a diagnostic workup, in which tomo functioned as a problem-solving modality for questionable cases detected on conventional DR, while positive cases went on for additional CT. Lead author Emilio Quaia, MD, and colleagues believe the diagnostic algorithm could reduce the number of unnecessary CT exams. The study was published June 30 in Academic Radiology.
The prospective trial involved 228 patients who underwent tomosynthesis and diagnostic CT after positive DR for pulmonary lesions. Practicing independently, two experienced radiologists first identified the suspected pulmonary lesions on DR (Definium 8000, GE Healthcare, Chalfont St. Giles, U.K.) that led to the decision to perform tomosynthesis with a commercially available system (VolumeRad, GE).
They then attempted to identify the same lesions and expressed their diagnostic confidence in the tomosynthesis images. The findings were confirmed with 64-slice CT (Aquilion 64, Toshiba Medical Systems, Otawara, Japan), which was also used for staging.
The researchers found that digital tomosynthesis cannot be considered without preliminary chest x-rays, but for both readers, the sensitivity, specificity, and diagnostic accuracy of the protocol improved significantly because of tomosynthesis.
For reader 1, the accuracy rates for DR and tomosynthesis were 43% and 90%, respectively. For reader 2, the accuracy rates were 49% and 92%, respectively. Receiver operator characteristics (ROC) analysis also indicated that the readers were significantly more confident in their interpretation of the tomosynthesis results than those rendered with conventional DR.
 |
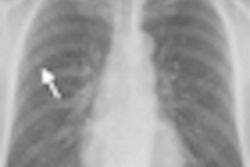
| Images of a peripheral lung nodule in a 65-year-old man. Posteroanterior radiograph (a) in the upright position shows one barely visible left lung nodule. Tomosynthesis image (b) shows the same nodule (arrow) as seen on the posteroanterior radiograph in (a) with a much higher conspicuity and with evidence of peripheral spiculations. CT image (c) (lung window, coronal plane reformation) confirms the left lobe nodule seen in (b) with evidence of peripheral spiculations. Images courtesy of Emilio Quaia, MD. |
Combined DR and tomosynthesis, however, were most likely to miss lesions less than 4 mm in diameter. The researchers also found that the combination can still contribute to the mischaracterization of extrapulmonary lesions. All 14 incorrect classifications by both readers in the trial involved extrapulmonary lesions that were misread as pulmonary abnormalities.
Reader 1 misinterpreted 10 pulmonary lesions viewed with tomosynthesis as pleural nodules, while reader 2 misread six pulmonary lesions as pleural nodules. All misses were in the anterior region of the lung parenchyma near the thoracic wall.
The differentiation between pulmonary and extrapulmonary lesions is crucial, Quaia said. Pulmonary lesions are contained within the lung and could require surgical or drug intervention if deemed malignant. Focal lesions of the pleura or thoracic wall are often benign and typically do not require therapeutic management.
Despite some limitations, the benefits of chest tomosynthesis are clear, according to Quaia.
"Digital tomosynthesis can be considered as a problem-solving technique to be employed in every patient with a doubtful or equivocal pulmonary lesion, based on the preliminary assessment of the digital chest x-ray examination," he wrote in an e-mail to AuntMinnie.com.
Pulmonary lesions confirmed on digital tomosynthesis and with a malignant pattern should undergo chest CT for staging, he noted. But CT is not indicated for overtly benign pulmonary lesions, pleural lesions, thoracic wall lesions, or pseudolesions characterized with tomosynthesis.
The judicious application of CT will spare some patients from unnecessary exposure to ionizing radiation, according to Quaia. The mean effective dose for CT depending on the tube current was 2-4 mSv. Digital tomosynthesis involved a 0.2-mSv dose, and a two-view digital radiograph exposed patients to 0.03-0.1 mSv.
The study's main limitation was the use of a heterogeneous group of patients who underwent chest radiography for varying clinical reasons, leading to a low incidence of malignant pulmonary lesions, Quaia said. The single-center nature of the trial was also a limiting factor.
By James Brice
AuntMinnie.com contributing writer
July 28, 2010
Related Reading
Will new DR technologies offer alternative to CT? Part 2, March 25, 2010
Will new DR technologies offer alternative to CT? Part 1, March 24, 2010
Low-dose tomo beats chest DR for TB evaluations, March 19, 2010
Virtual dual-energy DR improves lung lesion detection, February 10, 2010
Rads prefer dual-energy x-ray over standard DR in lung, January 29, 2009
Copyright © 2010 AuntMinnie.com