Fresh off the receipt of 510(k) clearance in August for its QCT Pro bone densitometry software, MindwaysCT is hoping to accomplish a goal that has long eluded healthcare professionals: increasing the dismal screening rate for osteoporosis by enabling the generation of bone density data from CT exams.
Screening rates for dual-energy x-ray absorptiometry (DEXA) have been stuck at about 20% of the at-risk population for decades. But MindwaysCT is aiming to move the needle north for at-risk people by offering screening almost automatically, using what it calls a "no dose" exam that can be performed retrospectively, long after the patient has been scanned, if necessary.
In fact, quantitative CT (QCT) screening can be performed with stored image data whenever a patient gets one of several kinds of CT scans, said Alan Brett, PhD, vice president of business development for MindwaysCT.
Analysis of QCT images for osteoporosis has been available for some time, but MindwaysCT's software generates T-scores for bone mineral density that are the same as those produced in phantom-calibrated QCT images -- and the same as scores produced by conventional direct x-ray DEXA exams.
The freedom to test for osteoporosis at any time using existing CT data comes from the fact that calibration phantoms no longer need to be in the CT picture, according to Brett.
"What it means is that you don't have to have the calibration phantom next to the patient," he said. "You can use CT scans that were ordered for different indications -- in the spine, the pelvis, [from] CT colonography, etc. Scanners are so stable these days that you can use your calibration data for months and years. So you don't need calibration per patient anymore, just per scanner."
The result is not only easier workflow, but the freedom to commandeer any noncontrast abdominal or pelvic CT in the patient's medical record for later screening without the patient's further participation in the process.
Patients at risk
This can be particularly synergistic for individuals undergoing CT colonography screening, Brett said. These patients are usually older than 50 and already at risk of osteoporosis, a particular concern among postmenopausal women.
"People who are having CT scans are very often having them for diseases that have consequences including bone loss; for example, a patient with inflammatory bowel disease almost certainly has bone loss going on," he said.
Other conditions that put people at risk include being on steroids or androgen deprivation therapy, as well as bone metastases. Chemotherapy and radiotherapy also lead to bone loss, though for these, the extent of damage is less clear.
"It's important because the consequences of osteoporosis are very severe [in terms of] morbidity and a high mortality rate," Brett said. "The International Society for Clinical Densitometry has numbers showing that less than 20% of women eligible for screening actually get a test, so the numbers are pretty low, and if you can get people tested from a CT scan, that can be very useful."
Reimbursement approved
Fortunately, Medicare will pay for QCT just as if it were a conventional DEXA exam, he said.
"Medicare will cover a bone densitometry screening exam for postmenopausal women every two years, so in theory any postmenopausal woman can get either a QCT or DEXA scan and have themselves tested for osteoporosis," Brett said.
The company's current clearance for the software, to be known as CliniQCT, is limited to CT of a few bones, including the lumbar region of the spine from T11 to T14, pelvis, femoral neck, and total hip.
The last two "are identical to DEXA measurements and designed to be the same as DEXA measurements. You get the same T-score out and you get real bone mineral density," Brett said. A paper in press by University of Wisconsin researcher Dr. Perry Pickhardt and colleagues shows a linear relationship between QCT and DEXA.
CTC/QCT combo ideal
Additionally, a successful pilot study published in 2011 focused on the feasibility of combining CT colonography (CTC) and osteoporosis screening (Journal of Computer Assisted Tomography, March-April 2011, Vol. 35:2, pp. 212-216).
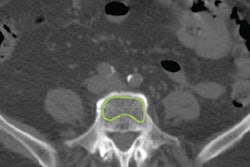
At the upcoming RSNA 2014 meeting in Chicago, Dr. Timothy Ziemlewicz, along with Pickhardt and other colleagues at the University of Wisconsin, will present a study of more than 130 asymptomatic adults older than 50 who underwent both osteoporosis screening and proximal femur QCT.
In this study, two-thirds of the cohort had never been screened for bone mineral density. But more than 30% of the subjects were classified as osteopenic, and close to 4.5% were considered osteoporotic based on QCT results, the study team will report.
Adding bone mineral density evaluation of the femoral neck to CTC allowed the researchers to identify a large proportion of patients with low bone mineral density who had not been previously identified.
"We plan to apply this to all CTs performed in patients eligible for bone mineral density screening -- regardless of indication -- so long as their referring physician wants the information," Pickhardt told AuntMinnie.com.
To leverage the synergies of CTC and QCT, the U.S. Centers for Medicare and Medicaid Services (CMS) would, of course, need to approve CTC reimbursement for colorectal cancer screening -- a process that has dragged on for years, with no resolution in sight.
"If we get [CTC] approved, then it seems to me that combining these two tests at the same time makes a lot of sense for patients and for Medicare," Brett said. Of course, Medicare would have to figure out how to pay for a combo exam in a scenario that lacks a clear precedent, he added.
For a disease with such high costs in morbidity and mortality, screening could produce huge benefits, Brett said. As for treatment, there are questions surrounding some of the existing pharmacological treatments, especially the older bisphosphonate drugs, but taking even simple steps toward treatment could make a huge difference in vulnerable populations.
"It would be worth being able to find patients who have low bone mass -- maybe not chronic yet -- and get them on exercise and calcium plus vitamin D," Brett said. "Anyone can exercise and eat better," he said, and some better but expensive pharmaceuticals are becoming available as well.