Focused abdominal sonography for trauma (FAST) exams can serve as a valuable triage tool in multiple casualty incidents (MCIs), according to researchers from Rambam Medical Center in Haifa, Israel.
"In the setting of a war-conflict-related MCI, integrating FAST as one of the first imaging methods during the continuous arrival phase is (prudent) triage," said Dr. Nira Beck-Razi. She spoke at the 2007 American Institute of Ultrasound in Medicine (AIUM) meeting in New York City.
In war, civilians and military personnel experience serious injuries that may be blunt or penetrating, and civilians may sustain blast injuries from bombs or missiles, Beck-Razi said.
To evaluate the role of radiologist-performed FAST as a triage tool for military and civilian multiple casualty incidents, the Rambam researchers retrospectively reviewed the records of 849 patients arriving at the level I trauma center during a one-month period during the Second Lebanon War in 2006. Of the total patients, 281 physically injured casualties were admitted, including 215 soldiers and 66 civilians.
Initial triage was performed at the emergency room entrance by the triage officer; FAST was performed on 102 (36%) of the admitted casualties, including 78 soldiers and 24 civilians, when an abdominal injury was suspected. Contrast-enhanced abdominal CT was performed in 68 of the 102 cases.
Three ultrasound scanners equipped with a 3- to 5-MHz transducer were placed in the emergency room for immediate performance of bedside FAST studies, which were undertaken by a resident or a senior radiologist.
Severe and moderate casualties with suspected abdominal injuries were the first to undergo FAST examination during the continuous arrival phase, Beck-Razi said. Based on the FAST results and patient hemodynamic stability, patients were prioritized for laparotomy, CT, or clinical observation, she said.
"Those who were positive for FAST and unstable went to laparotomy," Beck-Razi said. "Those who were negative for FAST but still unstable and had a strong suspicion of abdominal injury, they too went to surgery. The rest, whether positive or negative for FAST, that were stable went to CT, other examinations, and/or observation."
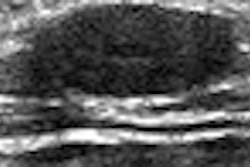
FAST findings were compared with the CT, surgery, and clinical observation records. The ultrasound findings were considered positive if free peritoneal fluid was present in any of the examined abdominal areas, Beck-Razi said.
Of the 102 FAST examinations, 17 (16.6%) were positive. Of the positive tests, there were two false positives. There were also five false negatives. Overall, FAST had a sensitivity of 75% and specificity of 97.6%, Beck-Razi said.
"You can see a strong correlation between FAST and the gold standards, which was defined as CT findings, laparotomy, and clinical observation records," she said.
While a slightly higher statistical value was obtained for the soldier group, the difference in FAST accuracy between civilian and military groups were not statistically significant (p = 0.38), Beck-Razi said.
FAST yielded a number of achievements, Beck-Razi said. For example, positive FAST studies in five hemodynamically unstable patients resulted in triage for stat surgery, she said.
"Due to the moderate sensitivity and the inherent limitation in diagnosing solid organs or hollow viscous injury, clinical judgment as always is crucial in unstable cases and in cases with a negative FAST," she said.
By Erik L. Ridley
AuntMinnie.com staff writer
June 20, 2007
Related Reading
Abdominal ultrasound aids dengue fever diagnosis, May 17, 2005
Ultrasound turns in middling results in blunt abdominal trauma, December 15, 2004
Experience beats speed in emergency FAST training, June 22, 2004
Emergency ultrasound training improves, but few ER docs meet AIUM guidelines, March 29, 2004
Copyright © 2007 AuntMinnie.com