Ultrasound may be able to differentiate between complicated and uncomplicated appendicitis, potentially helping physicians decide whether to proceed directly to an appendectomy or try antibiotics first, according to research published in the February issue of the Journal of Ultrasound in Medicine.
In a retrospective study of more than 100 patients, researchers from Stanford University found that one ultrasound finding -- the loss of the submucosal layer of the appendix -- produced 100% sensitivity and 92% specificity for complicated appendicitis.
"When ultrasound shows loss of the submucosal layer, complicated appendicitis is likely present and, therefore, surgery is likely to be necessary," senior author Dr. Eric Olcott told AuntMinnie.com. "On the other hand, when ultrasound does not show loss of the submucosal layer, antibiotics-first therapy can be considered."
Antibiotics first?
Patients diagnosed with appendicitis have traditionally been treated with an appendectomy. However, antibiotics are becoming more frequently considered as a first-line treatment, Olcott said (J Ultrasound Med, February 2017, Vol. 36:2, pp. 269-277).
"The choice of whether to do antibiotics-first therapy or surgery usually depends on defining whether appendicitis in a given patient is complicated -- meaning that the appendix is gangrenous or perforated and therefore antibiotics are unlikely to help -- versus uncomplicated -- patients whose appendices are not gangrenous or perforated, for whom antibiotics-first therapy is therefore more likely to be helpful," he said.
That determination of complicated versus uncomplicated appendicitis has typically been made using a variety of clinical, laboratory, and imaging criteria.
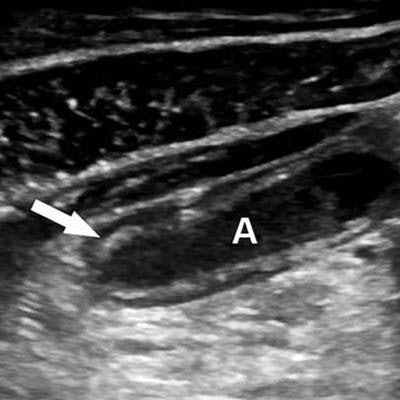
 Long-axis sonogram of the distal appendix (A) in a 14-year-old girl with uncomplicated appendicitis. Arrow shows complete preservation of the normal echogenic submucosal layer. All images courtesy of the Journal of Ultrasound in Medicine.
Long-axis sonogram of the distal appendix (A) in a 14-year-old girl with uncomplicated appendicitis. Arrow shows complete preservation of the normal echogenic submucosal layer. All images courtesy of the Journal of Ultrasound in Medicine.Ultrasound is used, with few exceptions, as the modality of choice at Stanford for pediatric and adult patients referred for imaging of clinically suspected appendicitis. As a result, the researchers wanted to investigate which, if any, ultrasound criteria could be useful for distinguishing complicated from uncomplicated appendicitis, helping to determine which patients could be considered appropriate candidates for antibiotics-first therapy.
An abdominal radiologist with more than 25 years of experience in grading-compression sonography of the appendix blindly reviewed the appendiceal sonograms of 119 patients with histopathologically proven appendicitis for sonographic findings such as the following:
- Loss of the submucosal layer: Defined as either focal or global lack of visualization of the normally echogenic layer, confirmed in both the long- and short-axis views of the appendix
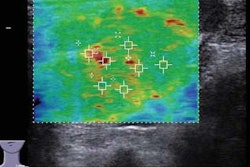
- Mural hyperemia: Diagnosed if at least 3 mm of contiguous color Doppler flow was identified in either long- or short-axis views
- Periappendiceal fluid: Diagnosed when localized fluid was identified immediately contiguous with the appendix
- Appendicolith: Diagnosed when an intraluminal echogenic focus was identified and cast an acoustic shadow
- Periappendiceal hyperechoic fat: Defined as hyperechoic tissue 1 cm or greater in size immediately adjacent to the appendix
- Measurement of the maximum outside diameter of the appendix: Measured from the outer wall to outer wall of the appendix in the short-axis view
The researchers compared those results with the presence or absence of complicated versus uncomplicated appendicitis as determined histopathologically. Of the 119 patients, 32 (26.9%) had complicated appendicitis; 21 had gangrenous appendicitis and perforation, while 11 had gangrenous appendicitis without perforation.
Loss of submucosal layer
After performing multivariate regression analysis, the researchers found that the loss of the submucosal layer was the only independent, statistically significant (p < 0.001) sonographic indicator of complicated appendicitis, yielding 100% sensitivity (95% confidence interval: 89.1%-100%) and 92% specificity (95% confidence interval: 84.1%-96.7%).
"Graded-compression sonography may, therefore, play an important role in identifying patients who are suitable for antibiotic-first therapy for appendicitis versus those who are suitable for appendectomy," the authors wrote.
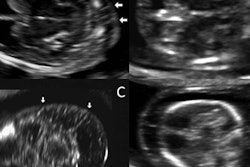
 Long-axis sonogram from a 19-year-old man with gangrenous appendicitis without perforation. Image shows global loss of the submucosal layer of the appendix (A).
Long-axis sonogram from a 19-year-old man with gangrenous appendicitis without perforation. Image shows global loss of the submucosal layer of the appendix (A).Olcott and colleagues acknowledged a number of limitations in their study, including the reliance on a single, experienced abdominal radiologist for the retrospective image review.
"Nonetheless the echogenic submucosal layer is a conspicuous finding such that loss of this reflector should be readily visible to less-experienced observers," they wrote.
Further, prospective studies will now be needed to further investigate the utility of the findings, Olcott said. In the future, the Stanford researchers plan to examine how these findings contribute to the management of patients with appendicitis.