Stereotactic body radiation therapy (SBRT) is effective in controlling the primary tumor of nearly 100% of patients with medically inoperable early-stage non-small cell lung cancer who are still alive three years after treatment, according to early findings of a North American clinical trial published today in the Journal of the American Medical Association.
The study's control rate is more than double the published rate of primary tumor control for similar patients who received conventional radiotherapy treatment, according to lead investigator Dr. Robert Timmerman in a press briefing this morning.
The three-year findings of the first North American multicenter cooperative clinical trial, Radiation Therapy Oncology Group [RTOG] 0236, testing stereotactic body radiation therapy were first presented at the American Society for Radiation Oncology (ASTRO) annual meeting in Chicago last November. The article, published in the March 17 issue of JAMA, provides detailed explanations of the treatment protocols and patient outcomes through August 2009 (Vol. 303:11, pp. 1070-1076).
Alternative to resection
Medically frail patients who have conditions such as emphysema and heart disease may not be able to tolerate anatomical resection, the standard treatment for early-stage lung cancer. Historically, they are offered 20 to 30 conventional radiotherapy treatments or are observed without specific therapy. Two-year reported survival for these patients is less than 40% with or without conventional radiotherapy treatment.
Stereotactic body radiation therapy instead uses highly focused, accurate beams of radiation to deliver radiation in one to five treatments to targets outside the brain. SBRT has been shown to work well in single-center studies, and Timmerman's RTOG 0236 phase II clinical trial wanted to test its efficacy in a multicenter environment.
The study's primary outcome was two-year actuarial primary tumor control. Secondary end points included disease-free survival, overall survival, and treatment-related toxicity.
Enrollment began in May 2004, with nine U.S. and Canadian cancer centers participating. Patients were required to be older than age 18 with biopsy-proven peripheral T1-T2N0M0 non-small cell tumors measuring less than 5 cm in diameter. Eligibility was limited to patients who were deemed surgically inoperable, who were not planning other types of treatment such as chemotherapy, who had not had prior radiotherapy to the thorax, and who did not have active systemic, pulmonary, or pericardial infection. Patients also became ineligible if they developed a synchronous malignancy within two years of enrollment.
A total of 55 eligible patients were enrolled before the study closed in October 2006. Of these, 62% were women, ranging in age from 48 to 89 years, with a median age of 72 years.
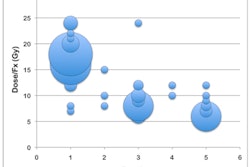
The patients received 60 Gy in three fractions of 20 Gy per fraction, prescribed to the edge of the planning target volume. (Due to overprediction of the actual planning target volume dose, the delivered dose was closer to 54 Gy in three fractions of 18 Gy.) The entire treatment needed to be completed within 14 days, with each treatment spaced a minimum of 40 hours apart.
Patients had follow-up appointments every three months during the first two years following treatment, and every six months for the next two years. The median follow-up for the cohort was 34.4 months, with a range of 4.8 to 49.9 months. Each patient had a CT scan at each follow-up visit to assess response and toxicity, and PET scans were required if progressive soft-tissue abnormalities were seen on the CT scans.
The researchers identified complete response as total solid tumor disappearance, and partial response was a decrease in the longest tumor diameter by 30% or greater, according to Timmerman, a professor of radiation oncology at the University of Texas Southwestern Medical Center in Dallas. Timmerman and colleagues defined primary tumor failure as evidence of tumor viability, marginal failures occurring within 1 cm of the planning target volume, and a 20% or greater increase in the longest diameter of the gross tumor volume confirmed by CT exam.
Of all the patients in the study, only one experienced a documented tumor recurrence or progression at the primary site. The three-year primary tumor control rate was 97.6%, and the three-year local-regional control rate was 87.2%. The authors noted that the control rate for conventional radiation therapy is typically 30% to 40%.
Three patients had recurrence with the involved lobe, and two patients experienced regional failure. Eleven patients experienced disseminated recurrence, at a 22.1% rate at three years following treatment. A total of nine patients experienced grade 3 (seven patients) and grade 4 (two patients) toxicities.
Twenty-six patients died, 10 of lung cancer. The research team reported that disease-free survival at three years was 48.3% and overall survival was 55.8%.
RTOG will be building on this clinical trial to design a trial to address what is considered to be a rather high rate of disseminated failure observed after treatment, complete a trial to determine a safe and effective dose for central lung tumors, and complete a trial to refine the dose of SBRT for peripheral tumors.
By Cynthia E. Keen
AuntMinnie.com staff writer
March 16, 2010
Related Reading
Adaptive radiation therapy monitors tumor change, December 25, 2009
Stereotactic radiotherapy effective in early inoperable lung cancer, April 20, 2009
High-dose stereotactic radiation effective for small lung metastases, March 26, 2009
Copyright © 2010 AuntMinnie.com