Young children with isolated lateral ankle injuries are often diagnosed with Salter-Harris fractures of the distal fibula, even if x-ray examinations do not reveal a fracture. But an MRI scan may change the diagnosis to a sprain, according to specialists at Toronto's Hospital for Sick Children.
The findings of a small prospective study conducted by a team of emergency, orthopedic, and radiology physicians suggest that Salter-Harris fractures of the distal fibula in children younger than 12 may be extremely uncommon (Injury, published online May 21, 2010).
More than 2 million children injure their ankles each year in North America. A Salter-Harris fracture of the distal fibula seriously restricts mobility, with immobilization for three to four weeks, and also brings limitations on weight-bearing activities, additional follow-up x-ray exams, and a follow-up consultation with an orthopedic surgeon as the recommended standard of care.
In the study, MRI scans were ordered for all children between 5 and 12 years old who had strong clinical indications of and were tentatively diagnosed with Salter-Harris fracture of the distant fibula at the hospital's emergency department during a 12-month period, commencing September 2008. Eighteen children met the study's criteria; the exams were ordered after negative three-view radiographs of the ankle, and they were performed within six days of the initial emergency department visit.
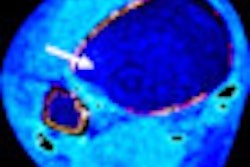
A fracture revealed on an MRI scan would have a distinct fracture line crossing the cortex and/or trabeculae, according to lead author and emergency physician Kathy Boutis, MD. The two radiologists who each independently reviewed the MRI exams could not identify any fractures based on this definition for any of the patients.
The radiologists determined that 16 of the children had MRI evidence of either a sprain and/or a bony contusion. Two children each had a subtle avulsion fracture and a minor articular cartilage injury. All MRI exams demonstrated edema overlying the lateral malleolus.
MRI exams should not be routinely ordered, due to their high cost, the authors cautioned. The injured children for whom an MRI was ordered represented fewer than 10% of patients who presented with ankle injuries during the time period of the study.
The authors acknowledged limitations of their study, including its small patient cohort and the fact that children younger than 5 were excluded because they would have required sedation with an MRI exam. For this reason, the authors recommended that further clinical research be conducted.
Related Reading
US overcomes x-ray's limits in pediatric ankle fractures, January 23, 2006
MRI can't replace x-ray for pediatric growth plate injuries, December 1, 2005
Pediatric ankle exam predicts need for x-rays, November 1, 2002
Copyright © 2010 AuntMinnie.com