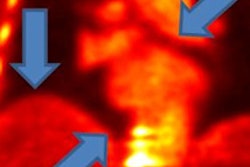
Simultaneous cardiac PET/MRI is better than PET/CT for detecting cardiac sarcoidosis, offering diagnostic image quality and less radiation dose, according to a study presented at RSNA 2015.
Preliminary findings showed that PET/MRI correctly diagnosed the inflammatory heart condition in all eight patients, compared with only four positive results with PET/CT. The additional information provided by PET/MRI could reduce the number of imaging exams patients undergo.
"Both PET and cardiac MRI are known to have diagnostic value in evaluating for cardiac sarcoidosis. So it seemed like a natural fit to use the combined modality to look for cardiac sarcoidosis," lead author Dr. Kate Hanneman, an assistant professor of radiology at the University of Toronto's joint department of medical imaging, told AuntMinnie.com.
Difficult to diagnose
Cardiac sarcoidosis is an inflammatory disease that can adversely affect heart function. Previous FDG-PET/CT studies have shown how inflammatory cardiac sarcoidosis can result in an increased risk of sudden cardiac death and onset of heart failure.
The challenge facing clinicians is that cardiac sarcoidosis is often very difficult to diagnosis.
 Dr. Kate Hanneman from the University of Toronto.
Dr. Kate Hanneman from the University of Toronto."Sarcoidosis most often involves the lung or the lymph nodes in the chest, which is more easily detected with CT," Hanneman said. "Cardiac involvement itself can be trickier to diagnose because it can be patchy and can involve portions of the ventricle that are not necessarily amenable to biopsy."
Previous research suggests that only approximately 5% of people who have sarcoidosis are identified as having cardiac involvement. However, prevalence of the disease may be closer to 25%, based on autopsy results.
"This discrepancy suggests that cardiac sarcoidosis involvement is probably underdiagnosed in clinical practice," Hanneman told RSNA attendees. "This largely relates to the fact that establishing a diagnosis is very challenging clinically, with the yield from endomyocardial biopsy at less than 20%.
Hanneman said it is not definitively known what causes sarcoidosis, and current imaging preferences to detect and diagnose the condition depend on the institution.
"Some centers rely more heavily on PET, while others rely more heavily on MRI," she added. "I don't think there is a clear consensus on which one is the most appropriate modality."
In the study presented at RSNA 2015, which Hanneman conducted during her fellowship at Stanford University, the researchers recruited eight consecutive patients (four men and four women; mean age, 53.3 ± 12.3 years) over a three-month period to assess for suspected cardiac sarcoidosis.
The patients were referred for a standard clinical evaluation with PET/CT and simultaneous PET/MRI. Prior to the scans, they were given eight-hour dietary instructions to suppress physiologic myocardial glucose uptake, particularly in the left ventricle.
Imaging protocols
The subjects first underwent standard cardiac PET/CT (Discovery 600 or 690, GE Healthcare) after injection of 9.7 mCi (± 0.4 mCi) of FDG. The scan was followed by a cardiac PET/MRI study using a simultaneous scanner with time-of-flight imaging on the 3-tesla MRI component (Signa, GE).
PET/CT was acquired with a delay of 92 minutes (± 26.6 minutes), while PET/MRI had a delay of more than 200 minutes (± 35.6 minutes) after FDG injection. Cardiac MRI sequences included breath-hold, electrocardiogram-triggered cine steady-state free precession (SSFP), T2-weighted, T1-mapping (pre- and postgadolinium-based contrast), and late gadolinium myocardial enhancement.
Total scan time for PET/MRI (75.8 ± 17.7 minutes) was approximately twice as long as with PET/CT (36.6 ± 6.3 minutes), due to the additional imaging sequences required for cardiac MRI. The patients handled the extra scan time with no issues, Hanneman noted.
'Interesting observations'
When paired with MRI, PET achieved positive cardiac sarcoidosis results for all eight patients (100%), compared with only four patients (50%) with the PET/CT combination.
This finding is "one of the more interesting observations" and may be due to a combination of factors, Hanneman said. One reason may be the newer generation of PET detectors on the PET/MRI system, which would enhance sarcoidosis detection.
"The second contributor is that we obtained the PET/MRI after the PET/CT, so there was a longer delay after the FDG injection," she added. "This longer delay may have allowed for greater FDG uptake. It is a point we want to study in the future."
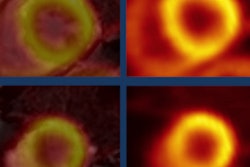
In addition, MRI was positive for sarcoidosis in six patients (75%), taking into account both late gadolinium enhancement and T2-weighted hyperintensity abnormalities.
Late gadolinium enhancement abnormalities alone were present in five patients (67%) and involved 10 myocardial segments, affecting 8% of the myocardium. T2 hyperintensity was present in four patients (50%) and involved five myocardial segments.
Patients also benefited from less radiation exposure with PET/MRI. The effective radiation dose from the CT component of the PET/CT exam alone was 4.6 ± 1.4 mSv, according to the researchers.
"These are preliminary results with a relatively small number of patients, so we have continued to recruit [more subjects]," Hanneman said. "It will be interesting to see how the results play out in the larger cohort of patients."
Hanneman received RSNA's Trainee Research prize for this paper.