A new cost-effectiveness model gives surprising prominence to the good old exercise treadmill test (ETT) for evaluating patients with suspected coronary artery disease. In fact, treadmill plus imaging -- especially coronary CT angiography (CTA) for low-risk patients -- was more cost-effective than any imaging modality alone, according to the study.
In its comprehensive examination of different diagnostic and treatment approaches to patients with suspected coronary artery disease, the study hypothesized that the low cost of ETT and the paucity of disease in low-risk populations combined to push initial treadmill testing to the forefront, despite its very modest sensitivity and frequently equivocal results.
The specter of fast-rising healthcare costs -- which currently consume 17% of the U.S. gross domestic product and are rising fast -- has focused a lot of attention on the high cost of attending to patients with suspected coronary artery disease, said Dr. James Min from Weill Cornell Medical College in New York City.
The cost of chest-pain evaluation alone has been tagged at more than $8 billion a year in the U.S.
"CT has been looked at in a number of prior studies to evaluate its cost-effectiveness in patients with suspected coronary artery disease," Min said in a presentation at the International Society for Computed Tomography (ISCT) meeting in San Francisco.
But those studies were all limited either by their small cohorts or their retrospective design, he said. Other efforts employed high-quality decision models, but simply didn't account for the full spectrum of imaging modalities and available treatment options.
The new study attempts to do it all by using a decision analytic model to evaluate the cost-effectiveness of coronary artery disease diagnostic strategies, as measured by incremental cost-effectiveness ratio (ICER) adjusted by life years, Min said.
"We tried to use the totality of commonly available and commonly utilized testing modalities including ETT, stress echocardiography, myocardial perfusion SPECT imaging [SPECT MPI] and CT angiography, and invasive coronary angiography," he said.
Using the option of applying successive noninvasive exams until a diagnosis is reached leaves 12 reasonable alternatives, all of which were modeled in the analysis:
- ETT followed by invasive coronary angiography (ICA) for equivocal or positive ETT (ETT-ICA)
- ETT followed by echocardiography for equivocal ETT and ICA for positive ETT (ETT-ECHO-ICA)
- ETT followed by myocardial perfusion scintigraphy (MPS) for equivocal ETT and ICA for positive MPS (ETT-MPS-ICA)
- ETT followed by coronary CTA for equivocal ETT and ICA for positive ETT (ETT-CCTA-ICA)
- Echocardiography followed by ICA for equivocal or positive echocardiography (ECHO-ICA)
- Echocardiography followed by coronary CTA for equivocal echocardiography and ICA for positive echocardiography (ECHO-CCTA-ICA)
- MPS followed by ICA for equivocal or positive MPS (MPS-ICA)
- MPS followed by coronary CTA for equivocal MPS or ICA for positive MPS (MPS-CCTA-ICA)
- Coronary CTA followed by ICA for equivocal or positive coronary CTA (CCTA-ICA)
- Coronary CTA followed by echocardiography for equivocal coronary CTA or ICA for positive coronary CTA (CCTA-ECHO-ICA)
- Coronary CTA followed by MPS for equivocal coronary CTA or ICA for positive coronary CTA (CCTA-MPS-ICA)
- Direct ICA
To model the postdiagnosis period, Min used a Markov model based on one-year cycles to account for outcomes and treatment costs for patients correctly diagnosed with coronary artery disease, the diagnosis of false negatives, and clinical events such as revascularization, all modeled from a payor perspective, he said.
"We looked at an economic model developed over a lifetime horizon," Min said. "We used ... test sensitivity and specificity, the rates of equivocal tests, and coronary artery disease prevalence in order to classify patients as true positives, false positives, true negatives, false negatives, or equivocal for obstructive coronary artery disease."
The model referred all positive results to invasive coronary angiography, which was assumed to have perfect sensitivity and specificity. Alternatively, patients could proceed to additional noninvasive testing, Min said.
Costs and quality-adjusted life years (QALYs) were calculated for all 12 diagnostic strategies, which were ranked by cost. Some strategies were eliminated by simple dominance (i.e., they were less effective and more costly than other strategies) and others were eliminated by extended dominance (i.e., the strategies were less effective than others and had a higher ICER).
The disease severity component of the model compared degrees of abnormality (none, mild, moderate, and severe) and functional measurements, as well as treatment implications, Min said.
Angiographic CAD (coronary artery disease) was defined for ICA and coronary CTA as absent, mild (1%-69% luminal narrowing), moderate (≥ 70% in one or two vessels, not including the left main artery), or severe (≥ 50% stenosis in the left main artery or ≥ 70% stenosis in three major epicardial coronary artery vessels). Post-test myocardial infarction patients were also deemed to have severe CAD.
Functional imaging CAD was applied to echocardiography and MPS. No CAD meant a lack of wall motion abnormalities or perfusion abnormalities. For mild, moderate, and severe disease, functional test results were deemed equivalent to angiographic severity, Min said.
ETT results for no CAD, moderate CAD, or severe CAD and equivocal results tied to exercise-induced ST-segment changes -- or the lack thereof. Patients ineligible for ETT (those with pacemakers, pre-excitation, 1 mm resting ST segment depression, etc.) were considered to have skipped the test, along with many patients in other groups who are unable to perform ETT.
Post-treatment approaches, following the results and recommendations of the recently published COURAGE and SYNTAX trials, included optimal medical therapy (OMT) alone for patients with mild CAD. They also included percutaneous coronary intervention plus medical therapy for 50% of patients with severe CAD, along with OMT alone for the other 50% of patients with severe CAD, Min said. Additional analyses were then performed for intermediate and conservative treatments.
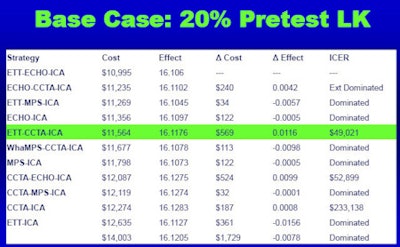
"We used a base case model of a 55-year-old man with stable chest pain syndrome and no prior history of CAD with a 20% risk of obstructive CAD, and we employed a common threshold standard of a $50,000 willingness to pay for discrimination of cost-effectiveness strategies," Min explained.
For this individual, treadmill test followed by coronary CTA when results were equivocal and ICA for a positive treadmill test "demonstrated a favorable ICER of $49,021 at 50% risk of obstructive CAD, ETT-CCTA-ICA cost $63,294 per QALY gained compared to the least expensive ETT-ECHO-ICA," Min said.
 |
| In low-risk patients with a 20% likelihood (LK) of disease, exercise treadmill testing, followed by coronary CT angiography, followed by invasive coronary angiography was the most cost-effective strategy, demonstrating an incremental cost-effectiveness ratio of $49,021. All data courtesy of Dr. James Min. |
"When we moved the pretest probability up to 50%," Min said, "you can see the red disappears because the cheapest strategy is the most cost-effective strategy, and that was treadmill testing, followed by stress echocardiography, followed by ICA."
 |
| In higher-risk patients with a 50% likelihood of disease, exercise treadmill testing, followed by echocardiography, followed by coronary angiography was the dominant strategy. |
"When we moved it up to 80% pretest likelihood, the cheapest strategy is treadmill testing, followed by nuclear testing, followed by cath, whereas the most cost-effective strategy is treadmill testing, followed by echo, followed by cath," Min said. At 80% risk, the ETT-ECHO-ICA strategy cost $38,234 per QALY, as compared to the least expensive ETT-MPS-ICA strategy.
 |
| In the highest-risk patients with suspected coronary artery disease (80% risk), exercise treadmill testing, followed by echocardiography, followed by invasive angiography cost $38,234 per quality-adjusted life year, whereas the cheapest diagnostic strategy was treadmill testing, followed by myocardial perfusion scintigraphy, followed by invasive coronary angiography. |
Beyond the initial diagnosis, different post-test treatment strategies also have a big impact on the effectiveness of postdiagnostic testing, Min said.
For intermediate-risk patients, the cost-effective strategy was treadmill testing, followed by CT when ETT was equivocal or couldn't be performed, followed by ICA. An aggressive post-test treatment strategy would favor treadmill testing, followed by echocardiography, followed by ICA, whereas extremely conservative management would favor coronary CTA first, followed by echocardiography for equivocal CT, followed by ICA, he said.
"In individuals with stable chest pain syndrome and suspected CAD, initial testing by ETT followed by imaging ... is more cost-effective than any strategy that employed initial testing by imaging alone," Min concluded. At lower and moderate risks of obstructive CAD, coronary CTA following ETT demonstrated favorable ICERs, while echo following ETT demonstrated favorable ICERs for higher-risk individuals," Min said.
Moreover, the post-test treatment strategy significantly affects the cost-effectiveness of diagnostic testing, he said.
Asked to suggest possible reasons for ETT's dominance among noninvasive tests, Min said that above all, ETT is inexpensive. Second, disease prevalence is so low in the low-risk cohort that it may be that even if ETT misses some disease, there are few poor outcomes to diminish its ranking.
By Eric Barnes
AuntMinnie.com staff writer
June 7, 2010
Related Reading
Coronary CTA best next test for positive stress patients, April 23, 2010
Zero calcium score enough to send chest pain patients home, February 10, 2010
Analysis favors coronary CTA over stress MPS for chest pain, January 15, 2010
ACCURACY trial compares coronary CTA to angiography, January 18, 2008
Coronary CTA results correlate with all-cause mortality, June 19, 2007
Copyright © 2010 AuntMinnie.com



















