A new analysis of data from the 2008 National CT Colonography Trial (ACRIN 6664) found no significant differences in the diagnostic performance of virtual colonoscopy in older individuals versus younger ones, researchers reported Wednesday in Radiology.
The positive data are renewing hopes among advocates of virtual colonoscopy (also known as CT colonography or CTC) that the exam might finally be moving closer to Medicare coverage.
The analysis of nearly 500 older subjects who participated in the 15-center ACRIN trial also found that adults 65 years and older were more likely to have a significant colorectal lesion, compared with younger participants. However, the total number of patients referred for optical colonoscopy would remain small (Radiology, February 24, 2012).
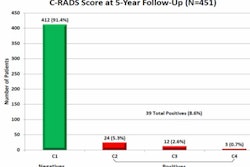
The results show that a vast majority of older screening subjects at average risk of colorectal cancer would be able to avoid screening optical colonoscopy, even if the polyp-size threshold for referral to invasive optical colonoscopy were as low as 6 mm.
"That means that about 87% of the patients who undergo CT colonography would not need to have subsequent colonoscopy to remove those polyps," said principal investigator Dr. C. Daniel Johnson, from the Mayo Clinic in Scottsdale, AZ, in an interview with AuntMinnie.com. "We'll identify those [with larger polyps] and they can be sent to colonoscopy."
The National CT Colonography Trial looked at 2,600 asymptomatic screening subjects at 15 U.S. centers and pegged CTC's sensitivity at 92% for adenomas 1 cm and larger -- a level equivalent to that of optical colonoscopy for detecting clinically significant lesions.
 |
| CTC endoluminal image of a 1-cm polyp attached to a colonic fold in the ascending colon. Image courtesy of Dr. C. Daniel Johnson. |
Nevertheless, the U.S. Centers for Medicare and Medicaid Services (CMS) in May 2009 deferred acceptance of CTC as a covered screening exam, citing a lack of data specifically demonstrating CTC's efficacy in older individuals, who represent the majority of Medicare beneficiaries. The present analysis was undertaken to address that shortage of data, joining a couple of other studies that yielded similar results.
The asymptomatic cohort was mostly at average risk for colorectal polyps and cancer in both the older and younger age groups. Among the older participants, 423 (89%) had no known colorectal cancer risk factors other than age, 35 (7%) had a first-degree relative with a history of colorectal polyps or cancer, 17 (4%) had a personal history of polyps or cancer, and two (0.1%) had both. All other participants were considered at average risk for colorectal cancer screening purposes. Overall, a medical history of polyps or colon cancer was more frequent in the older cohort (p < 0.001).
The analysis also found that older subjects had a few more extracolonic findings than younger participants, but none that required the addition of invasive procedures.
"The bottom line is that there was no significant difference in polyp detection for the two groups," Johnson said.
In their new study, Johnson and colleagues compared the sensitivity and specificity of CTC in participants younger than 65 years with results in those older than 65. Among the 2,600 asymptomatic screening subjects recruited for the original ACRIN trial, 497 (19%) were 65 years of age or older. That group, also led by Johnson, looked for clinically significant lesions 10 mm and larger as a primary end point, and measured the detection of smaller lesions (6-9 mm) as a secondary end point.
In its 2009 coverage denial, CMS was concerned about whether CTC's performance would be adequate in the older population because of factors related to exam performance. As a result, the new study was designed to focus on CTC's performance rather than polyp prevalence in that population -- and the results show that performance is equivalent, Johnson said.
"We did show an increased prevalence of polyps in this [older] population; therefore, the need for screening, in my mind, is even greater than in the population under age 65," he added. "But we know nationally that only about half of the population undergoes screening at the recommended intervals, so screening is really underutilized."
According to the results:
- Among the 477 older participants included in the new analysis, the prevalence of adenomas 1 cm or larger was 6.9%, compared with 3.7% for the younger group (p < 0.004).
- For large neoplasms, the mean estimate for CTC sensitivity was 82% and specificity was 83%. Among participants younger than 65 years of age, sensitivity was 92% and specificity 86%.
- Per-polyp sensitivity for large neoplasms was 75% for older individuals and 84% for the younger group. For lesions 6 mm and larger, per-patient sensitivity was 72% for the older group and 81% among younger patients.
The similar diagnostic performance shown in the analysis was particularly encouraging considering that the older subjects had a few factors working against them, including greater use of polyethylene glycol (PEG) preps. Distention was also slightly poorer among the older screening subjects, even though automated colonic insufflation with CO2 (ProtoCO2l, Bracco Diagnostics) was used in both age groups:
- A PEG prep was prescribed in a significantly larger proportion of older participants (n = 224, 47%) than younger subjects (n = 2,054, 39%). PEG preps can leave more residual fluid in the colon, potentially complicating interpretation of the images.
- Sodium phosphate, a drier prep preferred by many practitioners, was prescribed in a significantly smaller proportion of older participants (n = 225; 47%) than younger participants (n = 1,178; 57%).
- Optimal colon distention resulting in a well-visualized colon was found more often in the younger population (66%) than in older individuals (55%), a significant difference of 11%, and there were fewer "optimal" ratings for the amount of retained colonic fluid.
The slightly reduced distention quality in older screening subjects could be due to factors such as an incompetent ileocecal valve, poorer sphincter control, more advanced cases of diverticulosis and muscular hypertrophy, or more difficult patient rotation on the CT table, the authors wrote. Still, it's not necessarily a fixed disadvantage, they added. Distention issues, for example, can be managed by slower insufflation of the colon and vigilant review of the scout images before scanning.
Differences in type of colon preparation between the younger and older groups are not surprising because sodium phosphate is avoided in patients with comorbidities, especially those with cardiac and renal disease, the authors noted. Many providers avoid the use of sodium phosphate entirely. The PEG preparation is commonly associated with retained colonic fluid and is the likely cause of an increase in such retention. Retained fluid is a primary reason for the use of fluid tagging in the preparation protocol for all patients.
"Yes, colon distention wasn't as good because the older patients had more difficulty retaining the CO2 that we put in their colon," Johnson said. "Yes, the prep wasn't quite as good in the older patients as it was in the younger population. But the bottom line was whether we could screen these patients adequately, and I think really the proof is that there wasn't a significant difference in the polyp detection rate between the two populations."
The detection sensitivity differences between the populations weren't significant at either the 6-mm or 10-mm threshold, the study team reported.
Extracolonic findings were seen in 387 (81%) of the 477 participants 65 years and older, versus 1,278 (62%) of the 2,054 younger participants. Among the older screening subjects, 100 (21%) were deemed to require additional evaluation (including correlation with medical history or prior imaging) and four (0.8%) were said to need urgent care for at least one finding. By comparison, of the younger screening subjects, 15% needed additional evaluation and 1.3% needed urgent care.
There were two reports of adverse reactions in the older individuals, but both were thought to result from the conventional optical colonoscopy that each subject underwent prior to CTC.
 |
| Image republished with permission of RSNA, from Radiology, May 2012, Vol. 263:2, pp. 1-8. |
The analysis did not reveal significant differences in the diagnostic accuracy of CTC for detecting large and intermediate-size adenomatous lesions in participants 65 years of age and older, compared with younger participants, the study team concluded. Results in the average-risk cohort of patients older than 65 years "support virtual colonoscopy as a primary colorectal cancer screening tool for all eligible patients," the authors wrote. But the matter goes beyond affirming the adequacy of CTC as a screening exam, Johnson said.
"It really relates to the inadequate screening rates in the U.S," he said. "What we really want to do is get more people screened, and if we have more screening options, chances are we will screen more patients successfully and prevent more cancers from developing. [CTC] is an efficient way of trying to identify which patients go to colonoscopy, and it's also a way of providing access to additional types of exams so that patients are going to be screened more often."
The low-dose CTC protocol in the ACRIN trial led to radiation doses that were half the levels encountered in a standard abdominal CT exam (mean 6.9 mSv for both the prone and supine exam), Johnson noted. Even so, with the aid of iterative reconstruction and other dose-reduction techniques, CT technology has advanced since the 2008 trial results were published to the point where exams can now be acquired at approximately 25% of those levels, he said.
Finally, the biology of colorectal cancer is very favorable for cancer prevention compared to other diseases due to the long delay between the appearance of polyps and the development of cancer. As a result, the potential payoff resulting from increased screening is considerable, Johnson said.
"With breast cancer screening, we're looking for early cancers," he said. "With colon cancer screening, we can actually intervene earlier in the biology of these tumors at a time when they're not even malignant, and remove this really important class of cancers -- it's the second or third most common cancer killer in the U.S. today."
Dr. Perry Pickhardt from the University of Wisconsin, who participated in two previous studies analyzing CTC's effectiveness in older patients, which produced results similar to the current analysis, told AuntMinnie.com that the verdict is in regarding the use of VC screening in Medicare-aged individuals: It works.
"This study, along with larger series from our own institution [Kim, Pickhardt et al, Radiology, February 2010, Vol. 254:2, pp. 493-500] and the military experience [in press], removes perhaps the final hurdle for Medicare coverage of CT colonography for screening," Pickhardt said.