Korean radiologists found plenty of unsuspected lung cancers in a large cohort of patients being scanned for heart disease, according to a new study in Radiology. Most lesions were resectable, but most were seen only when the images were read using wider fields-of-view (FOV).
The study retrospectively evaluated the prevalence and radiologic features of lung cancer detected at cardiac CT, and compared detection rates at different field-of-view settings. The study is one of the first to examine the prevalence of lung cancer on cardiac CT scans, wrote Dr. Tae Jung Kim and colleagues from Seoul National University Bundang Hospital in Seongnam and Catholic University of Korea in Seoul.
"The clinical, radiologic, and histopathologic features of lung cancers detected at cardiac CT have not been addressed in detail previously," they wrote (Radiology, May 2010, Vol. 255:2, pp. 369-376).
The researchers scanned patients using either a 16-detector-row system (Mx8000-IDT, Philips Healthcare, Andover, MA) (n = 4,742 examinations) or a 64-detector-row scanner (Brilliance 64, Philips Healthcare) (7,526 scans) beginning at the level of the main pulmonary artery caudally through the entire heart.
Images were acquired at 16 x 0.75-mm collimation for the 16-slice scanner or 64 x 0.625-mm collimation for the 64-slice scanner, a gantry rotation time of 420-500 msec, a tube potential of 120 kV, and an effective tube current of 400-450 mAs at 16-slice imaging or 800 mAs at 64-slice imaging, following contrast administration with bolus tracking and a saline chaser. The mean radiation dose was 8.2 mSv ± 0.8 or 13.2 mSv ± 0.8 for 16- or 64-detector-row CT, respectively.
The results showed a lung cancer prevalence of 0.31% (36 positive cases) in the entire cohort of 11,654 patients. The positive cases included 16 patients (44%) who had never smoked, and researchers found a higher rate of cancer in patients suspected of having or known to have coronary artery disease (0.43%, 24 of 5,615 patients) compared to asymptomatic screening-examined patients (0.20%, 12 of 5,924 patients) (p = 0.0457).
 |
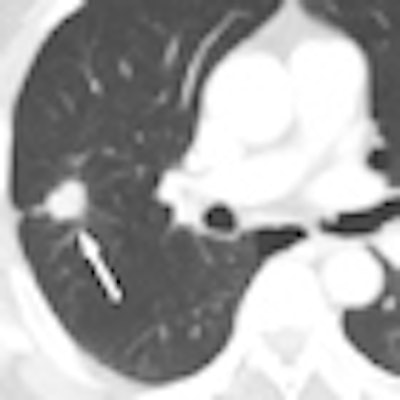
| Axial cardiac CT images in a 63-year-old man with solitary pulmonary nodule visible in full field-of-view only. Above, full-FOV image shows 2-cm spiculated nodule (arrow) in right upper lobe. Below, limited-FOV image obtained at same level shows nodule is collimated from view. This lesion was confirmed to be adenocarcinoma after right upper lobectomy. Images republished with permission of the Radiological Society of North America from Radiology (Vol. 255:2, pp. 369-376). |
 |
The mean diameter of the cancers was 23 mm ± 10.5 (range, 5-42 mm), and the most common location was the right upper lobe (n = 13, 36%). Adenocarcinoma was the most common histology, seen in 86% of patients (31 of 36) with lung cancer. Of the 34 non-small cell lung cancers detected at CT, 23 (68%) were resectable, including 16 of the earliest stage IA cancers, the authors wrote.
"The detection of lung cancer was significantly different between the limited- and full-FOV cardiac scanning examinations, between limited-FOV cardiac scanning and full-FOV thoracic scanning, and between the full-FOV cardiac and thoracic scanning examinations," the authors wrote (p < 0.0001 for all comparisons).
Importantly, of the 26 cancers detected at CT, four (11%) were seen with a limited FOV (covering the heart plus 1-4 cm). Meanwhile, 19 (53%) were seen with a wider FOV that extended from outer rib to outer rib and encompassed the entire lung parenchyma with the portion of the thorax that was imaged. Another 17 cancers (47%) could be detected only in full FOV at thoracic scanning, Kim and colleagues reported.
Cancer prevalence was comparable to that seen in recent low-dose CT trials for lung cancer screening, which ranged from 0.3% to 2.7%, depending on population characteristics including age, sex, and smoking history, the authors noted. However, the mean size of the lung cancers in the present study (23 mm) was larger than the 12-mm mean size in the Early Lung Cancer Action Program (ELCAP) and the 15-mm size found in the Anti-Lung Cancer Association (ALCA) study.
Cause for debate?
The authors acknowledged that their findings may add to the discussion over the extent to which cardiac scans should be examined for pathology outside the heart.
"There is ongoing debate as to whether the lungs and chest should be formally reviewed for extracardiac findings at cardiac CT," the authors wrote, citing Budoff and colleagues, who suggested that reanalyzing the data for extracardiac disease "would lead to additional costs and anxiety to patients, without proven benefits." However, several other authors recommend a thorough evaluation of the dataset. "It is well known that common symptoms of cardiac disease such as chest pain and shortness of breath are not universally accounted for by solely cardiac causes," Kim and colleagues added.
One thing is certain: A key point in CT's effectiveness in detecting extracardiac findings is in setting the imaging window wide enough to cover additional anatomy.
"Eighty-nine percent of lung cancers would have been missed with limited-FOV cardiac scanning," they wrote. "It is essential that the entire imaging dataset, including the full-FOV images, be evaluated at cardiac CT, because viewing in the limited FOV at cardiac scanning may result in the majority of lung cancers that could be detected on full-FOV images being missed."
By Eric Barnes
AuntMinnie.com staff writer
May 26, 2010
Related Reading
Accelerated RT improves lung cancer survival, May 3, 2010
CAD/PACS pairing boosts lung nodule detection, saves time, April 30, 2010
Lung group disputes CT screening study, April 29, 2010
CT-screened lung cancer patients live longer, May 11, 2009
NELSON lung cancer trial yields positive early results, March 9, 2009
Copyright © 2010 AuntMinnie.com



















