The American College of Cardiology (ACC) Foundation Task Force on Expert Consensus Documents has published the 2010 version of its views on coronary CT angiography (CTA) and cardiac MRI (CMR).
The documents were published online May 17 in the Journal of the American College of Cardiology and concurrently in several other publications. The documents emphasize the strengths and weaknesses of each technology based on literature and the writing committee's views.
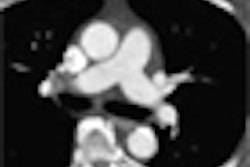
CT angiography
Studies indicate that coronary CTA could save time and reduce costs, particularly in lower-risk individuals who might otherwise receive additional tests, wrote Dr. Robert Harrington and colleagues. However, justification of coronary CTA remains less clear in other patient groups, they noted.
Also discussed were potential new applications for CTA including evaluation of plaque burden (for now, only research) and functional cardiac imaging exams, according to the writing committee.
Radiation was a central concern as the authors emphasized the need to conform to appropriateness criteria, especially for higher-dose exams. Radiation, as well as the contrast agents needed to perform so-called "triple-rule-out" imaging for chest pain, means CTA should only be considered when "clinical evaluation with targeted testing for the most likely causes" has not satisfactorily answered the clinical question.
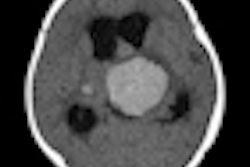
Cardiac MRI
In the CMR consensus document, also published online May 17 in JACC, W. Gregory Hundley and colleagues discussed the evolution and relative value of CMR over its principal alternative, cardiac CT, emphasizing the lack of radiation exposure to the patient.
They discussed the uses of dark and light blood imaging, late gadolinium enhancement, and the primacy of CMR for evaluating myocardial function. A major advantage of cardiac MR for evaluating myocardial mass and volume is its reproducibility and accuracy compared with 2D or planar projection techniques. Thus, cardiac MR can detect small changes in myocardial mass and/or volume that result from therapy.
Regional cardiac function can also be assessed with CMR, and "CMR can be used to assess myocardial metabolism without the need for administration of radioactive tracers," Hundley et al wrote.
Heart failure is an important application of CMR because it can address the presence and severity of morphological and functional abnormalities of the left ventricular or right ventricular myocardium, determining the underlying etiology of cardiac dysfunction.
Among CMR's advantages are its unique approaches to visualizing tissue pathology such as fibrosis; however, CMR remains technically challenging due to the small diameter of the coronary arteries and their constant motion.
The consensus document included a discussion of the latest views on the potential dangers of the magnet in the imaging suite, dangers in patients with implantable medical devices, and, finally, the risk of nephrogenic systemic fibrosis (NSF).
By Eric Barnes
AuntMinnie.com staff writer
May 19, 2010
Related Reading
JACC special issue tackles radiation dose in cardiac imaging, May 14, 2010
FDA changes PMA advisory panel process, April 27, 2010
NEJM study: Imaging procedures, radiation growing, August 26, 2009
ASE issues echocardiography contrast consensus statement, November 11, 2008
ACC/AHA issue new treatment guidelines for peripheral artery disease, December 7, 2005
Copyright © 2010 AuntMinnie.com