The presence of calcification on CT scans of thyroid nodules can neither prove nor rule out malignancy -- but calcification patterns may be one useful tool that radiologists can use to assess the likelihood of cancer, say researchers from China.
Calcification of thyroid nodules, regardless of pattern, suggests a higher risk of malignancy but is not definitive. And considering the number of incidental thyroid lesions detected at CT -- in as many as 8% of the adult population, at least 5% of which are malignant -- doctors can use all the help they can get.
Looking further into calcifications was the goal of a study presented at last month's International Congress of Radiology (ICR) in Shanghai. The small series focused on patterns in CT-detected thyroid nodules, which can be clues in determining malignancy, according to Dr. Wenli Tan and colleagues from Shanghai University of Traditional Chinese Medicine.
Finding other tools
Many patients who have thyroid calcifications detected on CT scans will require fine-needle aspiration, though elastography has also been proposed to help reduce the biopsy rate. Finding other tools for predicting malignancy is an important research goal.
The Chinese paper built upon previous research, including a 2008 paper from Korea that suggested that CT-detected calcifications have certain characteristics that can be used to predict malignancy. In the study, Yoon and colleagues looked at CT and ultrasound scans in 734 patients without known thyroid disease, searching for features suggestive of malignancy.
Yoon et al found that signs of malignancy could include nodular or rim calcifications (46.7% malignant versus 13.3% benign), an anteroposterior-transverse diameter ratio greater than 1 (33.3% versus 9.5%), and mean contrast-enhanced attenuation higher than 130 HU (86.7% versus 49.5%). The overall malignancy rate was 9.4% (Journal of Computer Assisted Tomography, September-October 2008, Vol. 32:5, pp. 810-815).
But Yoon and colleagues found no reliable criteria for malignancy in peripheral calcifications -- results that would contrast with those of the Chinese study.
Calcifications as malignancy predictor
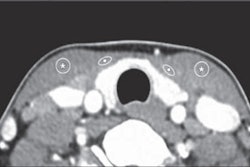
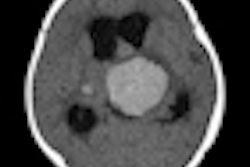
In the Chinese study, researchers examined 35 patients with calcified thyroid nodules proved by biopsy. They divided calcifications into "fine" (≤ 2 mm), "coarse" (> 2 mm), and "mixed" (both particle sizes by diameter). They also separated the findings by blurred or sharp borders, looking at density and enhancement values.
"Yoon et al suggested that there were no reliable criteria for malignancy in thyroid nodules with peripheral calcifications," Tan said. "In our study, calcifications of malignant nodules were in the center of the lesion with clear borders, which is consistent with previous studies."
There was also a statistically significant difference in the border calcifications, she said. Fourteen benign nodules had blurred border calcifications, while 12 malignant nodules had clear border calcifications.
|
|||||||||
| X2 = 30.2506, p < 0.0001 |
Microcalcifications had a high predictive value for malignancy (41.8%-49.2%) but low sensitivity (26.1%-59.1%).
|
||||||||||||
| X2 = 1.9679, p > 0.5 |
The diameter of the calcifications had no statistical significance for malignancy in this study, but that might be due to the way the calcifications were divided into fine, coarse, and mixed-particle lesions, Tan said. The rate of fine calcifications was 65% in benign lesions and 73% in malignant lesions.
|
Partial-volume effects in the 3-mm-thick scans were a limitation of the study, along with the small patient sample size, she said.
The researchers also found a statistically significant difference in the gender of the cases, with seven male patients who had malignant nodules and 28 female cases, Tan said. While the male-female ratio of malignant lesions was 1:1.5, among all lesions 85% were malignant in men versus 32% in women, she added.
|
|||||||||
| X2 = 4.5595, p < 0.05 |
"Thyroid nodules with calcification in males, thyroid nodules with blurred border calcifications, calcifications in the margin of the lesion -- all these characteristics suggest malignant disease," Tan concluded.
By Eric Barnes
AuntMinnie.com staff writer
May 12, 2010
Related Reading
Thyroid elastography may reduce unnecessary FNA biopsies, April 21, 2010
New ultrasound techniques show promise in thyroid nodules, February 5, 2010
Risk of thyroid cancer increased in childhood cancer survivors, October 28, 2009
ARRS study: US can help avoid thyroid biopsy, April 23, 2009
Screening for thyroid cancer worthwhile in some childhood cancer survivors, December 29, 2008
Copyright © 2010 AuntMinnie.com