SAN DIEGO - In what is likely the largest screening population ever classified by virtual colonoscopy's standardized reporting system, C-RADS, researchers found stable results over five years in the single-center program, along with a large majority of patients who were able to avoid invasive colonoscopy.
In a presentation on Wednesday at the American Roentgen Ray Society (ARRS) meeting, University of Wisconsin radiologists also said they saw a minor trend toward more follow-up imaging recommendations for extracolonic findings, which they speculate may be due to the addition of several readers.
"Standardized reporting is important in cancer screening, because it allows us to organize and categorize findings from institution to institution, so you can compare results between them," said Dr. David Kim, associate professor of radiology at the University of Wisconsin in Madison, in an interview with AuntMinnie.com.
Like BI-RADS for mammography, C-RADS (CT Colonography Reporting and Data System) is now used almost universally for screening exams, at least in all high-volume screening centers. The classification scheme ensures that practitioners are all speaking the same language, Kim said, and it enables meaningful comparison of data from the level of a single patient to the department and between imaging facilities.
The C-RADS reporting system, created in 2004 by a group of academic VC (also known as CT colonography or CTC) providers collaborating as the Virtual Colonoscopy Working Group, was published the following year (Radiology, July 2005, Vol. 236:1, pp. 3-9).
 |
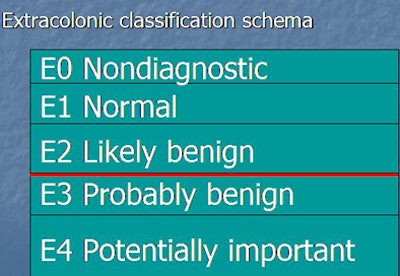
| Colonic classification schema (above) provides defined criteria that place an exam in a specific category, each with a defined management option. For C0 and C1, screening is recommended every five to 10 years beginning at age 50. For C2, evidence suggests that surveillance can be delayed at least three years, subject to individual patient circumstance. For category C3 and higher, subject to local practice, endoscopic biopsy may be indicated. In the extracolonic classifications (below), the important cutoff is between E2 (no further management indicated) and E3 (additional management recommended). All images courtesy of Dr. David Kim. |
 |
"It creates standardized categories for C [colonic] and E [extracolonic] findings and defines a standardized lexicon," Kim said.
The ARRS study reported a single center's experience with C-RADS, applied to a large average-risk cohort, which could provide expected benchmark values for screening CT colonography, Kim said in his presentation.
Colonic and extracolonic findings by C-RADS category
|
The cohort consisted of consecutive, average-risk patients referred by a primary provider for colorectal cancer screening.
It excluded subjects at high risk of colon cancer, including those with a history of bowel disease, polyposis syndrome, prior colonic resection, or prior surveillance. The mean age was 56.9 ± 7.3 years, and the cohort included more women (54.5%) than men.
A 6-mm polyp size threshold was used to define a positive exam, "and if there are multiple extracolonic findings, the exam was scored by highest-category finding," Kim said.
The men (n = 2,532) in the cohort had a higher overall proportion of positive (C2-C4) exams (15.4%, n = 362) than the women (10.5%, n = 295) (p < 0.0001), a finding Kim attributed to incidental adnexal/pelvic findings in women -- especially ovarian cysts.
In addition, positive exams (C2-C4) were more frequent in individuals 60 years or older (268/1,519; 17.6%) compared to those younger than 60 (389/3,654; 10.6%) (p < 0.0001).
To analyze trends over time, the group compared the results from the first 1,000 screening subjects to the last 1,000 -- or, actually, the last 1,173, as it turned out. While colonic findings were stable over the five-year period, there were statistically significant increases in recommendations for further follow-up among the extracolonic findings.
C (colonic) findings over time
|
E (extracolonic) findings over time
|
The combined categories E1 and E2 (no recommended action) dropped from 90.9% of the first 1,000 subjects to 84.8% of the last 1,173 (p < 0.001). The drop in normal findings roughly corresponds to the rise in E3 findings.
 |
| The percentage of normal extracolonic exams dropped between the beginning and end of the five-year period analyzed, corresponding to an increase in E3 categorization, which recommends additional imaging. |
Kim speculated on the cause of the upward trend in E3s, saying that because their radiology group is now larger, having trained additional radiologists over the five-year course of the program, these team members are bound to have individual approaches to categorizing the findings.
"You have more readers and perhaps different thresholds in deciding between E2 and E3, and the trend is that E3 is increased," he said. "But 12.3% [representing E3 findings with recommended imaging] is not a huge number, and what ultimately gets worked up decreases because some of the findings are already known, or given the clinical context of the finding, they choose not to work it up because doing so would not affect patient management."
Summarizing the results, Kim said that standardized reporting is important for CT colonography, allowing for comparisons of results at all levels. Most CTC exams in his institution are negative (86.4%) at the 6-mm threshold for positivity.
"There are positive associations with being male and over 60, and E3/E4 findings are associated with being female and over 60," Kim said. The percentages are stable for the colonic side and changing for the extracolonic side.
A minority of exams (11.6%) are categorized as E3/E4, requiring additional workup. Approximately 8% of all screening subjects at the facility are referred to same-day colonoscopy, he said.
"This study involves a large screening population to which C-RADS has been applied," Kim said. "It can provide values that a CTC program could expect in an asymptomatic screening cohort."
By Eric Barnes
AuntMinnie.com staff writer
May 6, 2010
Related Reading
Massive VC study yields trove of extracolonic cancers, March 23, 2010
VC screening maintains performance in Medicare population, November 9, 2009
VC in elderly patients yields extracolonic advantage, November 7, 2007
C-RADS reporting yields effective VC analysis, January 9, 2007
VC gets long-awaited reporting standards, November 2, 2005
Copyright © 2010 AuntMinnie.com