New research suggests that occult colonic perforation after incomplete optical colonoscopy may be more common than previously thought. The study, which recommends low-dose CT scanning of patients with incomplete colonoscopies before virtual colonoscopy (VC) is performed, could have important workflow and patient-safety implications in facilities that routinely perform same-day VC in patients with failed conventional colonoscopy.
Optical colonoscopy is considered incomplete when the colonoscope does not reach the cecum, a phenomenon that occurs in an estimated 3% to 23% of cases, noted study authors Dr. David Hough, Dr. Martin Kuntz, Dr. Jeff Fidler, and Dr. C. Daniel Johnson from the Mayo Clinic in Rochester, MN.
Virtual colonoscopy is commonly used to complete the colon exam after failed colonoscopy. The second exam is convenient because the patient does not need additional bowel preparation or a new screening appointment if VC can be performed later on the same day. Perforation, a known complication of colonoscopy, has been reported at rates ranging from one in 3,115 procedures (0.032%) to one in 510 procedures (0.196%).
"Very rare reports of colonic perforation at [CT colonography (CTC)] have emphasized that patients with obstructive lesions are at increased risk of perforation, and that approximately one-half of patients with colonic perforation as a result of CTC do not have symptoms," Hough and his team wrote. "The short time between incomplete colonoscopy and same-day or next-day CTC may not be adequate to allow some perforations to become clinically apparent" (American Journal of Roentgenology, October 2008, Vol. 191:4, pp. 1,077-1,081).
Due to the risk of exacerbating a clinically unsuspected perforation while insufflating the colon for VC, which can increase the risk of sepsis, screening for the presence of extraluminal gas before performing the exam may be beneficial, they wrote.
The study evaluated 262 patients (205 same day, 57 next day; 74 men, 188 women; mean age, 64 years; range, 21-92 years) with incomplete colonoscopies. Before the rectal tube was inserted and normal prone and supine VC images were acquired, the group underwent a special low-dose CT study specifically to look for evidence of extraluminal air indicating the presence of colonic perforation.
"The low-dose technique was determined semiempirically with the requirement that dose be as low as possible for maintenance of anatomic detail and visibility of gas," they wrote. "Images were reconstructed with 10-mm slice thickness at 10-mm intervals with a field-of-view to fit patient size."
Low-dose CT images were acquired at 2.5-mm or 1.25-mm collimation, 1.375 pitch, 120 kVp, and 40 mA on either an 8- or 16-detector-row scanner (LightSpeed Ultra 8 and LightSpeed 16, GE Healthcare, Chalfont St. Giles, U.K.). The normal settings for prone and supine VC are 120 kVp and 140 mA (8 x 1.25 mm) or 170 mA (16 x 0.625 mm).
"The total effective dose for the low-dose CT scan is approximately one-fifth the dose of single-pass standard CTC, or the equivalent of approximately 10 chest radiographic examinations," Hough and colleagues wrote.
Perforation was detected in two patients (0.8%; 95% CI, 0.1%-2.7%). The other 260 patients had uncomplicated VC exams with no perforation. The 262 incomplete colonoscopies included 166 (63.4%) screening colonoscopies, 39 (14.9%) surveillance procedures, and 57 (21.8%) diagnostic colonoscopies.
One patient with a perforation detected at low-dose CT was a 61-year-old woman undergoing screening colonoscopy. Tortuous anatomy prevented the colonoscope from being advanced beyond the proximal sigmoid colon. No symptoms were reported after incomplete colonoscopy, but the patient later mentioned having experienced nausea before and after the procedure. She was admitted to the hospital overnight and treated with IV fluids and antibiotics, and she experienced no further problems.
The second patient with perforation was a 70-year-old woman who had undergone screening colonoscopy. Acute angulation of the sigmoid colon prevented the colonoscope from being advanced more than 25 cm, and after five minutes of unsuccessful maneuvering it was removed. The patient had mild tenderness of the abdomen but no peritonism. She was admitted overnight and treated with antibiotics and IV fluids.
Overnight she developed worsening pain and a 38° C fever. "A diatrizoate meglumine and diatrizoate sodium solution enema examination the following morning showed no evidence of leak," they wrote. Symptoms resolved within 48 hours, and the patient was discharged from the hospital three days later with no further complications.
 |
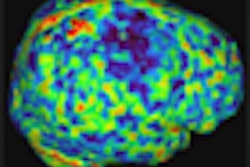
| Seventy-year-old woman who has undergone incomplete colonoscopy. Above and below: Axial CT scans of abdomen obtained before CT colonography show extensive retroperitoneal gas secondary to colonic perforation. Bottom image: Scout view from same examination shows extensive retroperitoneal air. All images courtesy of the American Roentgen Ray Society. Source: Hough DM, Kuntz MA, Fidler JL, et al. Detection of occult colonic perforation before CT colonography after incomplete colonoscopy: perforation rate and use of a low-dose diagnostic scan before CO2 insufflation. AJR. 2008;191:1077-1081. |
 |
 |
"We found that low-dose CT can depict clinically occult perforation before the patient undergoes CTC for incomplete colonoscopy," they wrote.
Evidence suggests that when a clinically unsuspected perforation occurs at colonoscopy, it is likely to be small and not clinically relevant. However, insufflating the colon in such patients before virtual colonoscopy risks exacerbating the perforation, the authors wrote. In comparison, the risk of a small additional radiation exposure after incomplete colonoscopy and before VC appears to be justified.
As for limitations, the study cohort was small, and the confidence index for the prevalence of clinically occult perforation after incomplete colonoscopy is wide, the authors wrote. Perforation also has been reported in rare cases following insufflation of the colon before VC undertaken without prior colonoscopy.
"Colonic perforation after colonoscopy can be clinically occult," the authors concluded. "We believe that our findings justify performing low-dose diagnostic CT before rectal tube insertion and gas insufflation in all patients referred for same-day or next-day CTC after incomplete colonoscopy in order to minimize the risks associated with exacerbating perforation."
By Eric Barnes
AuntMinnie.com staff writer
October 24, 2008
Related Reading
VC with automated insufflation effective in stenosing cancer. March 24, 2008
Automated CO2 insufflation edges patient-controlled air in VC, June 2, 2006
VC deflation maneuver reduces pain, November 21, 2006
Virtual colonoscopy shows favorable safety profile, May 5, 2006
Reading method, insufflation affect polyp measurements, November 4, 2006
Copyright © 2008 AuntMinnie.com