The New England Journal of Medicine today published results from the first large multicenter trial on the efficacy of virtual colonoscopy (VC or CT colonography [CTC]). VC's accuracy was comparable to that of optical colonoscopy for the detection of clinically significant colorectal polyps.
The results of the National CT Colonography Trial (ACRIN 6664) showed a per-patient sensitivity of 90% for the detection of adenomatous polyps 1 cm and larger. Detection sensitivity for smaller polyps, whose clinical significance is subject to debate, was somewhat lower.
In comparison, a study of back-to-back optical colonoscopies by Rex et al (Gastroenterology, January 1997, Vol. 112:1, pp. 24-28) found an overall miss rate of 6% for adenomas 1 cm and larger, yielding a sensitivity of 94%. Even so, adenoma detection rates can vary widely in colonoscopy, and significant numbers of studies are rendered incomplete when the colonoscope fails to reach the cecum.
Early results of the VC study, performed in 2,600 participants at 15 study centers across the U.S., were widely discussed and debated following their initial presentation at the American College of Radiology Imaging Network meeting in September 2007 in Arlington, VA.
Based in part on the early data, for example, the American Cancer Society elected in March to update its five-year screening guidelines to include virtual colonoscopy along with conventional colonoscopy and fecal occult blood testing (FOBT).
"The degree to which CT colonography is effective in detecting asymptomatic colorectal lesions remains a controversial topic, perhaps in part because of differences in patient populations, imaging protocols, and radiologists' qualifications in prior studies," wrote study author C. Daniel Johnson from the Mayo Clinic in Rochester, MN, and colleagues. "The National CT Colonography Trial of the American College of Radiology Imaging Network was designed to assess the accuracy of CT colonography in detecting histologically confirmed, large colorectal adenomas and cancers (≥ 10 mm in diameter), with optical colonoscopy (the current clinical standard for colorectal cancer screening) and histologic review used as the reference standard" (NEJM, September 18, 2008, Vol. 359:12, pp. 1208-1217).
Methods
The participants were recruited from patients 50 years of age or older who were scheduled to undergo routine colonoscopy, the authors wrote. Patients were excluded for symptoms suggestive of an elevated risk of colorectal cancer, such as rectal bleeding or abdominal pain, anemia, or a positive FOBT exam, or if they had undergone an optical colonoscopy exam within the previous five years.
The 15 U.S. sites included both academic centers and private practices, which recruited 2,600 asymptomatic outpatients who were scheduled for optical colonoscopy screening.
Training was an important component of the study, with VC readers required to have read at least 500 cases or have attended a 1.5-day training course. All had to pass a certified exam in which they detected at least 90% of the adenomas 1 cm or larger in 50 cases.
"Of 20 radiologists who met the initial entry criteria, the 15 with the highest scores on the qualifying examination were subsequently invited to participate in the study," wrote Johnson along with Mei-Hsiu Chen, Ph.D.; Alicia Toledano; Dr. Jay Heiken; Dr. Abraham Dachman; and colleagues.
VC data were acquired following standard cathartic bowel preparation with either polyethylene glycol (40% of participants) or sodium phosphate (55% of participants), stool and fluid tagging, and automated CO2 insufflation of the colon (ProtoCO2l, Bracco Diagnostics, Princeton, NJ). This was followed by additional mechanical insufflation of the colon if distension remained suboptimal.
Various CT scanners, all with 16 or more detector rows, were used in the 15 centers. Prone and supine imaging data were acquired using collimation of 0.5 to 1.0 mm, pitch of 0.98 to 1.5, matrix of 512 x 512, 50 effective mAs, and peak voltage of 120 kV. A standard reconstruction algorithm was used.
Following VC, optical colonoscopy and histologic review were performed; these served as the reference standard for the trial.
"The primary end point was detection by CT colonography of histologically confirmed large adenomas and adenocarcinomas (10 mm in diameter or larger) that had been detected by colonoscopy; detection of smaller colorectal lesions (6 to 9 mm in diameter) was also evaluated," the authors wrote.
Results
Complete data were reported for 2,531 (97%) participants. For large colorectal adenomas and cancers, the mean per-patient sensitivity, specificity, positive and negative predictive values, and area under the receiver-operating-characteristic curve for CT colonography were 90% (± 0.03%), 86% (± 0.02%), 23% (± 0.02%), 99% (± < 0.01%), and 89% (± 0.02), respectively, the authors reported. The per-polyp sensitivity for large adenomas or cancers was 84% (± 0.04%). The per-patient sensitivity for detecting adenomas 6 mm or larger in diameter was 78%.
"A single 10-mm cancer in the low rectum was missed on CT colonography," they wrote. "This lesion was not visible on a second review. A total of 30 lesions measuring 10 mm or more were detected in 27 participants on CT colonography but were not detected on the initial colonoscopy. Fifteen of these 27 participants, with 18 reported lesions, returned for a second colonoscopy, as called for by the protocol. Five of 18 lesions were confirmed on the second colonoscopy (considered to be true-positive CT colonographic findings)."
The study data were randomly assigned to be read independently using either primary 2D or primary 3D search methods. Various workstations were used to interpret the data, including InnerviewGI (Vital Images, Minnetonka, MN), Advantage CTC (GE Healthcare, Chalfont St. Giles, U.K.), syngo Colonography (Siemens Healthcare, Malvern, PA), V3D Colon (Viatronix, Stony Brook, NY), and Aquarius (TeraRecon, San Mateo, CA).
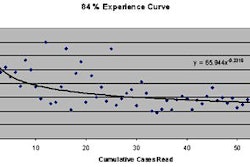
"The pooled sensitivities for detecting large lesions with the use of primary two-dimensional conventional software and primary three-dimensional endoluminal fly-through software were similar: 0.87 (95% confidence interval [CI], 0.75 to 0.95) and 0.88 (95% CI, 0.76 to 0.95), respectively," the group wrote. "The difference between the two types of viewing software was not significant. The mean time was 19.4 minutes for the primary two-dimensional interpretation, as compared with 25.3 minutes for the primary three-dimensional interpretation. There was no correlation between the number of cases interpreted and the radiologist's performance."
Adverse events were reported in three participants. One had severe nausea and vomiting for less than 24 hours after VC. Another had hematochezia after snare polypectomy, requiring two days of hospitalization. A third participant was hospitalized for Escherichia coli 24 hours after VC and colonoscopy.
The researchers found extracolonic findings in 66% of participants, of which only 16% were deemed important enough to require further evaluation or urgent care.
"In our study, CT colonography identified 90% of patients with asymptomatic large colorectal adenomas or cancers (≥ 10 mm in diameter) that were detected by optical colonoscopy, with an AUC [area under the curve] of 0.89," Johnson and colleagues wrote. "Secondary analyses showed that CT colonography had a lower sensitivity for smaller colorectal lesions (6 to 9 mm)."
Most VC trials have yielded lower detection sensitivities than the current study. One that produced better results, by Pickhardt et al (NEJM, December 4, 2003, Vol. 349:23, pp. 2191-2120), relied on primary 3D interpretation of the data.
"Although the higher accuracy in the study by Pickhardt et al has been attributed by some to the use of a primary three-dimensional endoluminal reading technique, our study showed similar performance with the two image-display methods and all software brands used," the authors wrote. However, the primary 2D interpretation required nearly six additional minutes (a 23% increase) in interpretation time compared with primary 3D. The mean time was 19.4 minutes for the primary 2D interpretation, as compared with 25.3 minutes for the primary 3D interpretation.
"Despite the consensus opinion that colorectal cancer screening is effective, adherence to current guidelines remains low among adults eligible for screening," Johnson and his team wrote. "Guidelines for colorectal cancer screening support multiple test options so that patients and providers can work together to determine their preferred method of examination. The less invasive nature of CT colonography and the low risk of procedure-related complications, as compared with colonoscopy, may be attractive to patients and may improve screening-adherence rates by addressing certain concerns of both patients and providers."
CT colonography identified 90% of patients with adenomas and cancers measuring 10 mm or more in diameter, they concluded.
'An excellent test'
"Overall, this study corroborates our earlier findings that CTC is a safe and effective test for colorectal screening of average-risk adults," commented Dr. Perry Pickhardt, an associate professor of radiology at the University of Wisconsin Medical School in Madison, who was not involved in the study. "There is now overwhelming evidence that CTC represents an excellent test -- perhaps the best test -- for colorectal cancer screening and prevention. Coverage of CTC screening by third-party payors such as Medicare should be just around the corner."
Less enthusiastic was an editorial accompanying the NEJM study by Dr. Robert Fletcher, professor emeritus at Harvard Medical School in Boston. Fletcher wrote that while the study results help put colorectal cancer screening "on more solid ground," concerns remain about the cumulative effects of the radiation dose, if CTC is to be conducted regularly at five-year screening intervals for individuals age 50 and over.
"In addition, CT colonography may miss some flat or depressed adenomas, which comprise about 10% of precancerous adenomas," he wrote. " These concerns do not rule out CT colonography as a screening test but they need to be considered, as do the consequences of the other screening-test options, including colonoscopy, when CT colonography is chosen" (NEJM, September 18, 2008, Vol. 359:12, pp. 1285-1286).
By Eric Barnes
AuntMinnie.com staff writer
September 18, 2008
Related Reading
American Cancer Society recognizes virtual colonoscopy screening benefit, March 5, 2008
ACRIN trial shows VC ready for widespread use, September 28, 2007
Radiologists eye VC practice post-ACRIN, February 10, 2007
Gastroenterologists plan to perform VC, January 25, 2007
New data reveal higher efficacy for primary VC screening, October 18, 2006
Copyright © 2008 AuntMinnie.com