The jury has not yet rendered a verdict on the value of thin-section CT slices in colorectal polyp detection, but the lengthy trial is at least moving forward. Among the questions presented in cross-examination: Does tighter longitudinal resolution really improve the ability to find lesions in virtual colonoscopy? And if so, are the additional findings the ones that radiologists really need to see?
A pair of recent studies examined the case in different ways. From Stanford University in Stanford, CA, Padmavathi Sundaram, Ph.D., Dr. Christopher Beaulieu, Dr. David Paik, and colleagues wanted to know if a computer-aided colonic polyp detection system could tell the difference between thin and thick collimation in a phantom. It could, at least among the smaller polyps.
And from New York University in New York City, Dr. Yvonne Liu, Dr. Michael Macari, and Dr. Gary Israel and colleagues sought to evaluate differences between thin- and thick-section reconstruction of MDCT colonography data in patients, as interpreted by radiologists. Thin sections improved specificity, but not sensitivity.
These groups weren't the first to ask the question. Dr. Cynthia McCollough and colleagues from the Mayo Clinic in Rochester, MN, for example, used a colon phantom and an MDCT scanner to determine the optimal scanning protocol. They found that thin-section and noise-reduction techniques were not needed to visualize polyps larger than 10 mm (Abdominal Imaging, May-June 2002, Vol. 27:3, pp. 253-259).
In a follow-up study, the air-filled phantom was scanned at different slice thicknesses ranging from 1.25 to 5 mm, and different x-ray tube currents ranging from 5 to 308 mAs. All polyps were detected in all the datasets except for one. At 1.25 mm slice thickness and an extremely reduced mAs of 5, image noise reduced polyp visibility, and five of 140 (3%) polyps could not be identified, the authors wrote (Abdominal Imaging online, October 28, 2003).
And in another phantom study presented earlier this year, Dr. Johann Wessling and colleagues from the University of Muenster in Germany found that thicker slices may distort the appearance of smaller polyps and inhibit their detection in virtual colonoscopy, though tube-current changes did not affect detection. A more detailed discussion was subsequently published in Radiology (September 2003, Vol. 228:3, pp. 753-759).
Finally, Ling et al from George Washington University in Washington, DC, used a phantom and a CAD scheme to look for "polyps," all larger than 10 mm, using eight different scanner settings. Five-millimeter collimation made detection more difficult, but the group concluded that clinically significant polyps could be detected with 100% sensitivity in all orientations, doses, collimations, and modes used in the study (Journal of Computer Assisted Tomography, November-December 2002, Vol. 26:6, pp. 1,013-1038).
Stanford researchers weigh in
Sundaram's group used a CAD scheme, a phantom, and a single patient to test a range of exposures, looking for polyps of all sizes.
"Studying this...will enable us to better understand the improvements in detection sensitivity resulting from decreasing slice thickness," they wrote. "It will enable us to better understand the improvements in detection sensitivity resulting from decreasing slice thickness. It will also enable us to turn CAD polyp detectors to effectively detect a particular size range of polyps. We expect that just as the tradeoff between noise and longitudinal resolution made by choosing a given slice thickness affects the human detectability of small structures, a similar effect will be evident for CAD algorithms. The purpose of our study is to quantify the effect that the choice of slice thickness has on the performance of a specific CAD algorithm under clinical conditions."
An air-filled water phantom complete with simulated haustral folds was used to perform CT imaging, using collimation settings of 1.25 mm, 2.5 mm, 3.75 mm, 5 mm, 7.5 mm, and 10 mm. The same range values were used for the 50% overlapping reconstruction slice thicknesses, as well as table speeds (in mm per 360°).
Virtual colonoscopy was also performed on a single patient, a 56-year-old woman. Prone and supine images were acquired using an eight-slice scanner (LightSpeed Ultra, GE Medical Systems, Waukesha, WI), at 4 x 1.25 mm, 12 mAs, and 120 kVp, with 50% overlapping slices reconstructed at the same 1.25-mm, 2.5-mm, 3.75-mm and 10-mm intervals.
The surface normal overlap CAD detection scheme (presented at the 2002 RSNA meeting by Paik, Beaulieu, and colleagues) was used to evaluate both the phantom and human datasets. Free response receiver-operating characteristics (FROC) curves plotted for each different z resolution, and contrast-to-noise ratios were studied as a function of slice thickness and polyp size.
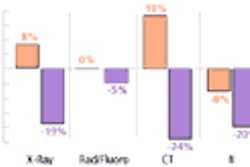
According to the results, reducing the slice thickness from 5 to 1.25 mm improved sensitivity from 84.5% to 98.3% for phantom polyps of all sizes, and from 61.4% to 95.5% for those ranging in size from 0-5 mm, at a constant false-positive rate of 20 per dataset. In the 5-10-mm range, reducing slice thickness from 5 mm to 1.25 mm improved sensitivity from 84.5% to 98.3%. Predictably, reducing slice thickness did not significantly improve sensitivity for polyps 10 mm and larger.
Similarly, in the prone and supine patient data, detection sensitivity gradually dropped with reductions in z resolution, from a total of 113 polyps in the single patient (12 larger than 10 mm, 57 5-10 mm, 44 smaller than 5 mm). At a false-positive rate of 20, improving the z resolution from 5 to 1.25 mm causes the sensitivity to increase from 20.5% to 27.3% for polyps smaller than 5 mm. But for polyps larger than 10 mm, at the same false-positive rate, the same improvement in z resolution does not improve sensitivity, Sundaram and colleagues wrote.
The contrast-to-noise ratio varied predictably with slice thicknesses for different polyp sizes, but in all cases remained high at > 4, and the phantom results were similar to those for the patient.
"We found that the performance of the CAD polyp detector consistently improves with decreasing slice thickness, even as noise increases," they wrote. "We therefore conclude that for the performance of the CAD polyp detector, noise is a less important factor than contrast, which improves with thinner slices."
Among the study limitations discussed, the authors cautioned that their results might not necessarily correspond to those of other CAD schemes. "However, the results of our CAD algorithm rest entirely on the results of edge detection, which is quite general, since most of the other CAD polyp detectors use gradient information in some way."
Moreover, there is no a priori reason that optimization for both CAD and human readers should be the same, they noted, adding that CNR settings should be optimized for the two tasks independently.
"In conclusion, we found that improving z resolution in general improves the sensitivity of the computer-aided polyp detector," the authors wrote. "But the gain in sensitivity depends strongly on the size range of polyps being detected relative to the slice thickness. For polyps larger than 10 mm, there is no improvement in detection sensitivity by reducing slice thickness."
NYU study finds higher specificity with thinner slices
A recent study from New York University examined different reconstruction parameters in 25 patients who underwent virtual colonoscopy, followed by conventional colonoscopy used as the reference standard.
"Investigators in two recent studies used multidetector-row CT to evaluate different aspects of this technology: Hara et al used a 4 x 5-mm detector configuration to increase acquisition speed, while Macari et al used a 4 x 1-mm detector configuration in conjunction with a high pitch value to optimize section profile," Lui and colleagues wrote (Radiology, May 2001; Vol. 219:2, pp. 461-465; and Radiology, August 2002, Vol. 224:2, pp. 383-392, respectively).
Unfortunately, they added, radiation dose issues prevent the comparison of different section thicknesses in the same patient, but once data were obtained with normal thicknesses they could be subjected to a variety of thin- and thick-section reconstructions.
In the study, 25 male patients (50-76 years) underwent virtual and conventional colonoscopy following purgative bowel cleansing. CT images were acquired using a Somatom Plus 4 Volume Zoom multidetector-row CT system (Siemens Medical Solutions, Malvern, PA). Images were acquired in a single breathhold at detector collimation of 4 x 1 mm, 120 kVp, 0.5-second gantry rotation, 50 effective mAs, and pitch of 6-7.
Images were reconstructed using two methods: 1.25 mm (thin) sections reconstructed every 1 mm; and 5-mm sections (thick) reconstructed every 2 mm. Two independent readers blinded to patient information and colonoscopy results examined the images. They relied on primary 2-D interpretation using a transverse cine technique on a Vitrea 2 workstation (Vital Images, Plymouth, MN). Each reader interpreted all of the thin-section datasets first. After a minimum 15-day wait, they each interpreted all of the thick-section images in a different patient order.
Fifteen of the 25 patients had normal findings, and the remaining 10 patients had 12 polyps (5 mm and smaller n=7; 6-9 mm n=2; 10 mm and larger, n=3). Sensitivity was the same for both readers in every polyp size range.
Using thin sections, sensitivity for the detection of polyps was 43%, 100%, and 100% for polyps 5 mm and smaller, 6-9 mm, and 10 mm and larger, respectively. Using thick sections, sensitivity was 29%, 100%, and 100% for the same size ranges.
"Overall sensitivity was 66.7% for thin sections and 58.3% for thick sections; the decline in sensitivity was not statistically significant (P=0.299)," they wrote. "The 95% confidence indices of the sensitivity difference between the thin and thick sections were 0 and 20.8."
Thin-section imaging produced three false positives (all for Reader 1), each measuring 3 mm. Thick sections left Reader 1 with six false-positive findings. Reader 2 had 6 false positives with thin-section imaging and 11 with thick sections. The number of false-positive findings was significantly lower for thin-section imaging compared to thick-section imaging for both readers (P=0.035).
As for specificity, Reader 1 had 93.3% with thin sections and 80% with thick sections. Reader 2 had 80% specificity with thin sections and 73.3% specificity with thick sections.
However, mean interpretation times were significantly longer for thin-section imaging. Mean times for Reader 1 were 11 minutes ± 1.4 (SD) for thin sections and 8.6 minutes ± 1.2 for thick sections. Reader 2 spent a mean time of 13 minutes interpreting both thin and thick sections; however, the standard deviation was 5.6 minutes for thin sections and 4.7 minutes for thick sections.
"In the present series on the comparison of thin- and thick-section CT colonography, our findings demonstrate no difference in per-polyp sensitivity by using thin vs. thick-section reconstructions," the authors wrote. "Most small polyps were missed, and all lesions larger than 6 mm were detected...These small lesions would likely be detected at follow-up screening if there was substantial growth."
However, the number of false-positive findings was lower with thin sections than with thick sections. For virtual colonoscopy to be widely accepted, it is extremely important to decrease the number of false positives, lest such findings lead to unnecessary further tests, the authors wrote. And even though the use of thin-section reconstructions increased mean interpretation times for Reader 1, the 13-minute mean time was not excessive. Also, while thin-section imaging produced a trend toward improved specificity, it did not reach clinical importance, the authors wrote.
"When comparing thin and thick sections at CT colonography, our preliminary observations suggest that there is no difference in sensitivity," they concluded. "Specificity was improved for both readers by using thin-section CT, and there were substantially more false-positive findings detected with thick sections than with thin sections."
By Eric BarnesAuntMinnie.com staff writer
November 26, 2003
Related Reading
Thin slices, narrow collimation rule in virtual colonoscopy study, March 8, 2003
Researchers settle on 'best' CT protocol for multislice virtual colonoscopy, September 25, 2003
Copyright © 2003 AuntMinnie.com