This article originally appeared in the American Journal of Roentgenology, written by Dr. Howard Forman, associate editor of health policy for the American Roentgen Ray Society (ARRS).

In this brief, I will summarize the three main sources of concern for practicing radiologists -- both academic and private: the Deficit Reduction Act of 2005, passed into law in early 2006; the sustainable growth rate legislation, passed into law in 1997 (Balanced Budget Act of 1997); and the five-year review of physician work relative value units, announced by the Centers for Medicare and Medicaid Services (CMS) on June 21, 2006.
The Deficit Reduction Act (DRA) of 2005
In January 2007, unless otherwise repealed or modified, outpatient imaging practices will find their technical reimbursement reduced to the lesser of hospital outpatient reimbursement or the physician fee schedule, effectively reducing and capping the technical fees for most diagnostic imaging. In fact, only mammography (screening and diagnostic) was expressly excluded from this provision. The same act reduces the technical fee for multipart imaging studies (i.e., when an abdominal CT and a pelvic CT are done in one imaging encounter, there will be a fee reduction instead of paying the full technical component for both).
This reduction has already begun phasing in, reaching maximum effect in January 2007. These changes will significantly affect practices, particularly those that rely on outpatient imaging. The one positive note in this act was a reversal in the expected reduction of all physician fees as part of the sustainable growth rate legislation (see below).
The sustainable growth rate (SGR) legislation
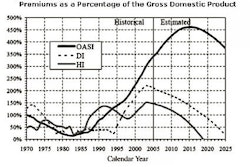
Almost every physician has read or heard about SGR at one point or another. This important piece of legislation, embedded in the Balanced Budget Act of 1997, was intended to slow the growth in Part B Medicare by modifying the physician fee schedule to account for increased (or decreased) utilization by beneficiaries. The assumption was that physicians would restrain use of services and keep their per-case reimbursement up or would suffer if Medicare beneficiary utilization was above trend. Ultimately, this was an effort to reduce the costs of the Part B program, which is 75% funded out of the general revenue of the U.S. government.
Determining the physician fee schedule update is based on a two-step process. First, CMS estimates the "sustainable growth rate" for the given year. This is a combination of the projected changes in input prices for physician services, real gross domestic product (GDP) per capita (which is the only major allowance for growth in utilization), enrollment in traditional Medicare fee-for-service, and spending attributable to changes in law and regulation. For 2007, the estimate is for an SGR of 0.7%. The savvy reader will quickly realize that this "allowance" makes no account for improvements in technology or advancement in illness severity. Thus, it was always expected to hold down utilization or reimbursement. Since physicians seem unable to really hold down utilization, reimbursement has suffered.
The second step in the process involves determining the actual update to the physician fee schedule. This is a function of the change in input prices for physician services and an update adjustment factor that allows total physician services to meet the sustainable growth rate target over time. Even when Congress temporarily (as they have in all but one of the past seven years) suspends the impact of the SGR legislation, the actual target is not changed and, thus, the subsequent year's adjustment factor is that much deeper.
When one uses all of the best current estimates, the update for physician fees in 2007 is estimated to be -4.6%. Worse still, the actual update factor for 2007 was -28% (a result of all of the previous years' reversals). Statutorily, however, the maximum adjustment factor in a given year is 7%, which when combined with the change in input prices, yields the -4.6% figure.
This is a rather dramatic problem to address. While Congress has the ability to override this change with legislation, it has thus far been unwilling to repeal the overall law, leaving all physicians and their patients at risk for the future. Further, when Congress does decide to do an "annual fix," as it has done, it frequently marries it to something draconian, as seen in the Deficit Reduction Act of 2005 (see above). In that act, the dramatic reimbursement changes to radiology practice were tied to a reversal of the 4.4% reduction in the fee schedule (which was modified to be a 0% update).
CMS' five-year review
Every five years, CMS reviews the actual weighting and work units attributed to each billable item. The recently released proposed changes will have a substantial impact on radiology, though variable across subspecialties. In general, the update is expected to increase reimbursement to emergency medicine, family practice, and internal medicine, while reducing reimbursement to anesthesiology, dermatology, pathology, and radiology (5% reduction as of January 2007). In addition, practice expense reforms were also submitted (and to be phased in over a four-year period), yielding a modest 2% improvement in reimbursement to our practices. Also note that these do not include the SGR update, so the predicted actual reduction could be quite high.
When one reviews individual CPT codes, the effect can be quite dramatic. As currently predicted (including all changes noted above, but not including the SGR cuts), the technical component of some important imaging procedures, such as MRI of the face/neck/orbits with and without intravenous contrast and lumbar spine examinations with and without intravenous contrast, may see 20% or more reductions. For certain add-on heart-imaging codes, the decreased technical component reimbursement from Medicare is greater than 50%! Even the simple chest radiograph will see a technical fee reduction of approximately 15%. On the other hand, there are substantial increases in technical components of CT of the abdomen and pelvis and MRI studies of the lower extremities.
Overall, the five-year review would seem to adversely affect the technical component more than the professional component, but as noted, this varies by the mix of cases in your practice.
Managing the potential crisis
When one scrutinizes the many expected changes in radiology reimbursement set forth in this brief, a certain sense of caution or fear may be warranted. Historically speaking, in most years Congress does ameliorate the SGR cuts; on the other hand, the other revisions tend to take hold with minor modification. The changes that are coming to our practices are targeted at every aspect of our professional lives: all techniques; all types of practices; and differing, but significant, effects on professional and technical reimbursement.
There are two main ways to manage this potential crisis: Prepare for the cuts and look to additional means to improve productivity. The impact of technology on our practices is certainly being felt in a positive way and there is still room for more improvement. Further, the recent introduction of radiology assistants bodes well for our practices.
Encourage your federal representatives to address this problem. Even though mammography was specifically excluded from the DRA reductions, it is not safe from the SGR updates or other revisions to the fee schedule. Beneficiary access to breast imaging and all other important services must be emphasized.
Finally, I think it is worth noting that managed care and commercial payors very often follow the lead of Medicare, so practices that are less reliant on Medicare should not feel safe. The leaders of our specialty are speaking out about these proposed reductions, but active involvement from residents, faculty, and private practice clinicians will be necessary to defer or reverse these major changes.
By Dr. Howard P. Forman
AuntMinnie.com contributing writer
August 21, 2006
Forman is an associate editor of health policy for the American Roentgen Ray Society (ARRS). This article originally appeared in the American Journal of Roentgenology (August 2006, Vol. 187:2). Reprinted by permission of the ARRS.
Related Reading
Medicare 2006 and beyond: What comes after 'critical'? July 25, 2006
Offshoring, teleradiology, and the future of our specialty, March 20, 2006
Copyright © 2006 American Roentgen Ray Society