A low-dose coronary CT angiography (CTA) technique known as adaptive statistical iterative reconstruction (ASIR) can reduce the radiation dose associated with coronary CTA by 27%, according to a study published online August 20 in the American Journal of Roentgenology.
The proprietary iterative reconstruction method, which got its initial clinical testing in body imaging, was also a stellar performer in coronary CTA that substantially reduced radiation doses in a large patient without any degradation in signal, noise, or signal-to-noise ratio, according to researchers who scanned patients at two Canadian centers and one U.S. center.
"ASIR permits the use of lower tube current with similar image noise and study interpretability in comparison with coronary CTA studies performed with [filtered back projection (FBP)] and higher tube current," wrote lead study author Jonathon Leipsic, MD, from the University of British Columbia and St. Paul's Hospital in Vancouver, and colleagues.
Compared to FBP, "ASIR makes fewer assumptions regarding the distribution of noise and utilizes an iterative process of mathematic modeling to identify and selectively reduce noise," they explained.
Iterative reconstruction techniques, including the ASIR implementation (GE Healthcare, Chalfont St. Giles, U.K.), have been introduced in the past couple of years as image reconstruction algorithms for CT that provide an alternative to traditional filtered back projection.
While FBP is fast and requires less time and computational power to perform than other reconstructions, images reconstructed using ASIR have lower image noise.
"ASIR uses iterative comparisons of each acquired projection to a synthesized projection incorporating modeling of both system optics and system statistics, permitting more efficient image updating," Leipsic and colleagues explained. "Because of its noise reduction capability, ASIR in theory can be used to reconstruct images with similar image quality (noise and signal-to-noise ratio) but with a substantial reduction in tube current, resulting in a reduction in overall radiation dose."
 |
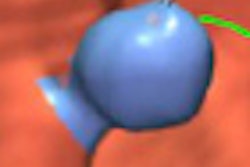
| Effect of ASIR on image signal and noise. CT angiographic images show ascending aorta in 48-year-old man. Images were reconstructed using both FBP (left) and 40% ASIR (right). Window width and level are the same for each. Signal and noise measurements were taken from 1-cm2 circular region of interest in same location. Signal was similar between FBP and ASIR (718.6 HU versus 719.3 HU, respectively), whereas noise decreased between FBP and ASIR (52.3 HU versus 38.5 HU). All images republished with permission of the American Roentgen Ray Society. |
The researchers scanned 574 consecutive patients undergoing coronary CTA at the three centers. Scanning parameters included a rotation time of 350 msec, 64 × 0.625-mm collimation, tube voltage of 100 or 120 kV, and tube current of 275-800 mA, adjusted for the patient's body mass index. To minimize the radiation dose, sequential scanning with minimal padding was used whenever medication enabled a heart rate of 65 bpm or less, unless a retrospective acquisition was needed to evaluate the left ventricle.
Two of the sites used a triple-phase contrast protocol that included 60 mL of iodixanol (Visipaque, GE Healthcare), followed by 75 mL of a 50:50 mixture of iodixanol and saline, then a 50-mL saline flush. The third center used a dual-phase protocol with 75 mL of iodixanol followed by a 50-mL saline flush, according to the authors.
Comparisons were performed between consecutive groups initially using FBP and subsequently using ASIR, with regard to patient and scan characteristics, radiation dose, and diagnostic study quality.
The studies were interpreted on an Advantage Workstation (AW 4.3-4.4, GE Healthcare) by three experienced coronary CTA imaging specialists, each with experience in several thousand studies. They rated diagnostic study quality both per artery and per segment, and every anatomically present segment 1.5 mm or larger was evaluated for diagnostic quality. Images were reconstructed using 0.625-mm slice thickness.
The 574 patients (mean age, 56 ±13 years) consisted of 331 who received FBP and 243 who had ASIR. The groups were demographically similar except that ASIR patients were more likely to be male.
There were no differences between groups in the use of prospective gating, tube voltage, or scan length, but scans performed using ASIR had a lower median tube current than those acquired using FBP (median [interquartile range], 450 mA [350-600] versus 650 mA [531-750], respectively; p < 0.001).
In addition, ASIR-acquired images were associated with a 44% reduction in the median radiation dose compared to FBP (4.1 mSv [range, 2.3-5.2] for FBP versus 2.3 mSv [range, 1.9-3.5] for ASIR; p < 0.001).
After adjustment for different scanner settings, ASIR exams were associated with a 27% reduction in radiation dose compared with FBP (95% confidence interval: 21%-32%; p < 0.001). Nevertheless, there were no significant differences in adjusted signal (p = 0.61), noise (p = 0.73), or signal-to-noise ratio (p = 0.19) between the two methods. There were no differences in interpretability.
 |
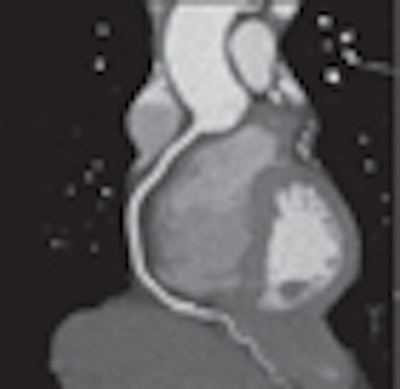
| Images of patient at normal weight: 55-year-old woman who presented with chest pain (body mass index, 22 kg/m2). Scanning parameters were 100 kV, 325 mA, 0 msec padding, and scan length of 13.9 cm. Effective radiation dose was 0.56 mSv. Left anterior descending (left) and right coronary (right) arteries are displayed with curved multiplanar formations without stenosis or visualized plaque. |
"Our study results show that ASIR permits reduction in tube current while imparting a statistically significant reduction in radiation dose due to the direct relationship between tube current and dose," Leipsic and colleagues wrote.
The effect of this dose reduction is incremental to other dose reduction methods in use, and although tube current reduction in CT would be expected to result in increased image noise due to the decreased number of photons, "the studies reconstructed with ASIR had no significant increase in image noise when compared with the FBP studies," they wrote.
Study limitations included the use of a nonrandomized study cohort; interpretations blinded to the image-reconstruction method were not possible. In addition, each exam was interpreted by a single experienced reader. Finally, the ASIR algorithm was implemented only on a newer scanner model (Discovery CT750 HD, GE Healthcare) that uses a more advanced detector, which may have contributed to improvements in image quality independent of the effect of the ASIR algorithm.
"To our knowledge, this study represents the first validation of the new ASIR algorithm as a radiation dose reduction tool in coronary CTA," the team wrote.
ASIR allows the use of lower tube currents with similar image noise and study interpretability compared to coronary CTA studies performed with FBP and higher tube currents. "ASIR represents a novel method of radiation dose reduction that appears additive to existing techniques," they concluded.
By Eric Barnes
AuntMinnie.com staff writer
August 20, 2010
Related Reading
ASIR halves VC dose without drop in image quality, June 21, 2010
MBIR aims to outshine ASIR for sharpness, CT dose reduction, May 18, 2010
Filtering software boosts CT image quality, lowers dose, May 7, 2010
Reduced dose can still yield acceptable pediatric CT images, April 22, 2010
ASIR cuts dose in Crohn's disease patients, December 4, 2009
Copyright © 2010 AuntMinnie.com