VIENNA - Studies continue to show the value of coronary CT angiography (CTA) in individuals at high risk of coronary artery disease, but its value in individuals at intermediate risk is unclear.
Just last week, researchers from Detroit reported that 64-slice CTA provided the correct diagnosis in 95% of patients with low-risk acute chest pain.
Today, at the cardiac imaging sessions of the European Congress of Radiology (ECR) researchers from Austria reported that CTA is not only warranted for individuals in the middle of the Framingham risk profile, but that it saves money compared to other diagnostic modalities.
Previous studies have demonstrated high accuracy for CTA in patients with significant stenoses greater than 50%, said Dr. Gudrun Maria Feuchtner from Innsbruck Medical University in Austria.
"However, these studies have not selected patients with a high probability of coronary artery disease," she said, "so the purpose of this study was to assess the diagnostic accuracy, and also the clinical value, and perform a cost analysis of patients at intermediate risk in the Framingham profile."
Feuchtner presented her group's study of patients at intermediate risk, including individuals with atypical chest pain, and asymptomatic individuals with inconclusive/equivocal or mild-pathologic ECG stress tests.
Of the 106 subjects (mean age 58 years), "20% (n = 21) were asymptomatic and 80% (n = 85) had atypical angina-like chest pain," typically cardia and a feeling of pressure in the chest, but not radiating pain "and not reproducible or constantly occurring in exercise," she said. "ECG stress test findings were either mild-positive or borderline positive for ischemia or suggestive for coronary heart disease, or stress test results were not evaluable, limited, or some even normal," or equivocal. ECG stress test results were inconclusive in 21 patients and mild-pathologic in 22.
Coronary CTA was performed on a 64-slice Sensation scanner (Siemens Medical Solutions, Erlangen, Germany) following administration of 90-110 mL of contrast media, either iodixanol (Visipaque 320, GE Healthcare Bio-Sciences, Chalfont St. Giles, U.K.) or iomeprol 400 (Iomeron, Bracco Diagnostics, Princeton, NJ) at a fast 5 mL/sec using bolus tracking.
Images were acquired at 64 x 0.6-mm collimation, 0.33 sec rotation speed, 120 kVp, and 900 mAs. The effective slice thickness was 0.75 mm. Retrospective ECG gating was performed at 30% or 70% of the RR interval, depending on heart rate.
Invasive coronary angiography was used following CTA only when clinically indicated, in 17 of the 106 patients.
The results showed that "the vast majority of patients had coronary artery disease, defined as the presence of coronary plaques, in 68% (n = 73), and out of those, 10% (n = 7) had only noncalcified plaques, a calcium score of zero," Feuchtner said.
The prevalence of significant coronary stenosis, defined as greater than 50%, was low at 7.5% (n = 8) of patients, but 33% (n = 35) had nonsignificant stenosis at CTA, she said.
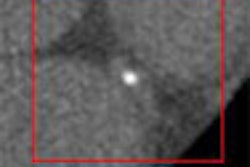
In a male patient presenting with atypical chest pain, normal ECG stress test results, and nonreproducible chest pain attacks, CT revealed a stenosis of more than 50% in the left anterior descending artery, a proximal noncalcified plaque that was confirmed by invasive coronary angiography, Feuchtner said.
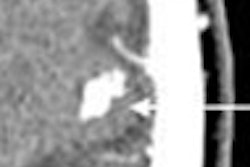
In another patient, a young man with multiple risk factors who presented with atypical chest pain attacks and nonspecific ECG stress test findings, CT correctly showed an 80% stenosis of the left anterior descending artery. However, CT was false-positive in the same patient's right coronary artery, one of two false positives in the study that occurred in patients with severe calcifications.
CTA's diagnostic accuracy was comparable to previously published literature, with 100% sensitivity for the detection of stenosis greater than 50% per patient, specificity of 77.8%, positive predictive value of 80%, and negative predictive value of 100% compared with invasive coronary angiography, Feuchtner said.
As for the cost analysis, Feuchtner and her colleagues based it on the actual costs to the hospital for a coronary CTA exam at her hospital, about 215 euros ($282 U.S.), and the cost of invasive angiography, at about 1,180 euros ($1,548) per exam.
"After selecting only patients … in whom two cardiologists would have recommended angiography if CT had not been available, the CT ruled out in 17 of 22 significant coronary artery disease, resulting in a savings of 20,060 euros ($26,311)," she said.
Outcomes at one year were uneventful in 17 of those patients, and the other five were referred for angiography, resulting in two false positives and two true positives. Adding in the cost of those exams, the use of CTA saved about "18,000 euros ($23,609) if angiography is used as a second-line invasive test," according to Feuchtner.
CT's image quality was acceptable in 78% of the studies, limited in 19 patients and inadequate in just one patient whose heart rate increased after the scan was initiated, she said.
"In summary, 64-slice CT performed well in patients with an intermediate Framingham risk profile for excluding coronary artery disease, and utilizing 64-slice CT as a gatekeeper for invasive coronary angiography may also be cost-effective, at least it saves actual costs" in these patients, Feuchtner said.
In response to a question following her talk, Feuchtner said her group also detected a small number of incidental findings, mostly small lung nodules, but did not include costs associated with following up incidental findings in the study design.
By Eric Barnes
AuntMinnie.com staff writer
March 10, 2007
Related Reading
MDCT offers cost-effective, reliable diagnosis in low-risk angina patients
Calcium scoring requires individualized reconstruction phases, March 5, 2007
Radiation dose slashed in 64-slice coronary CTA, February 15, 2007
64-slice CT takes on dual-source in cardiac radiation dose, January 26, 2007
Inflammatory view: Imaging blind to plaque risk, December 7, 2006
Copyright © 2007 AuntMinnie.com