Coronary CT angiography (CTA) outperforms calcium scoring for predicting short-term outcomes, say Michigan researchers. Three months after the scans, coronary CTA was head and shoulders above calcium and other risk factors as a prognosticator of major adverse cardiac events.
In symptomatic patients referred for coronary CTA, the presence of coronary artery calcium (CAC) came in a distant second to CTA, followed by Framingham risk factors, the group reported at the recent Society of Cardiovascular Computed Tomography (SCCT) meeting in Orlando, FL.
"We know the prognostic value of calcium scoring, which has been published in multiple studies," said lead investigator Dr. Kavitha Chinnaiyan in an interview with AuntMinnie.com. "What we wanted to see was how much incremental value was obtained by adding CT angiography to the calcium score. We took short-term outcomes; we still need to evaluate intermediate- and long-term outcomes."
The retrospective study examined 1,568 patients (mean age, 55 ± 12 years; 53% men) who underwent CAC scoring and coronary CTA at the hospital in addition to a complete three-month follow-up.
"We looked at all downstream hospital [care] and major adverse cardiac events," including death and acute coronary syndromes, Chinnaiyan said. After scanning, the study tracked patients' hospitalizations, emergency department evaluations, stress tests, invasive coronary angiography (ICA) procedures, and revascularization procedures (percutaneous coronary intervention [PCI] and/or coronary artery bypass graft [CABG] surgery), according to Chinnaiyan, who is director of cardiac imaging education at William Beaumont Hospital in Royal Oak, MI.
Following the results of CAC scoring and coronary CTA, the 1,568 patients were stratified into one of four groups based on their Agatston CAC score and the percentage diameter of coronary artery stenosis detected at CTA, as follows:
- CAC ≤ 400 + stenosis ≤ 50% (group 1) - (n = 1,245, 79.4%)
- CAC ≤ 400 + stenosis > 50% (group 2) - (n = 171, 10.9%)
- CAC > 400 + stenosis ≤ 50% (group 3) - (n = 50, 3.2%)
- CAC > 400 + stenosis > 50% (group 4) - (n = 102, 6.5%)
Gated calcium scans were performed just before retrospectively triggered coronary CTA using a 64-detector-row scanner (Somatom Sensation 64, Siemens Healthcare, Malvern, PA) or a Siemens Definition dual-source scanner, Chinnaiyan said.
Prospective gating is now routinely used for patients with steady heart rates and no arrhythmias, she said. And, as the result of a new statewide dose-reduction program initiated at the facility, even retrospectively gated exams are being performed at an average radiation dose of 6 to 8 mSv.
Chinnaiyan and colleagues Dr. Michael Walls, Dr. Ryan Madder, and Dr. Aiden Abidov, Ph.D., performed a stepwise-forward multivariable analysis to assess the incremental prognostic impact of coronary CTA findings over both clinical data and CAC.
"As we go up in the groups from 1 to 4, there was a gradual increase in all risk factors -- importantly, group 1 [CAC ≤ 400 + stenosis ≤ 50%] had lower risk than any of the other three groups combined," whereas in the higher-numbered groups, "patients are older, they have more traditional risk factors, such as diabetes and high blood pressure, and more patients have peripheral vascular disease," she said.
 |
| In the 1,528-patient retrospective study, those in groups 3 and 4 tended to be older and present with more risk factors than patients in groups 1 and 2 (groups are in order from left to right in the table). However, group 2 patients, despite having fewer risk factors, had the highest rate of major adverse cardiac events, hospitalizations, percutaneous coronary interventions, and combined major adverse cardiac events. All images courtesy of Dr. Kavitha Chinnaiyan. |
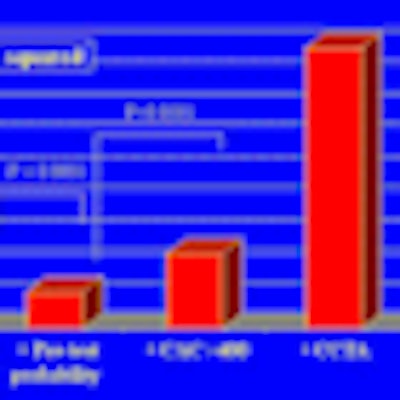
At multivariable analysis, stenosis severity assessed by coronary CTA was the strongest independent predictor of major adverse cardiac events, with significant incremental value over the combined effect of all clinical variables and CAC.
At three months, "the greatest number of events occurred in patients with stenoses greater than 50% -- and the calcium score didn't matter," Chinnaiyan said. "So regardless of whether they had a calcium score of zero, the [presence of stenosis] really drove downstream events, hospitalizations, and revascularizations."
 |
| Outcomes three months after a coronary calcium scan show a higher rate of adverse events and hospital utilization for patients with significant stenosis, regardless of calcium score (ED = emergency department, ICA = invasive coronary angiography, PCI = percutaneous coronary intervention, CABG = coronary artery bypass grafting, RU = resource utilization, MI = myocardial infarction, MACE = major adverse cardiac events). |
Even when patients with stenosis less than 50% had events serious enough to be defined as major adverse cardiac events, the events tended to be less serious than those in patients with stenoses greater than 50%, she added.
For example, despite the presence of fewer risk factors, patients in group 2 (CAC ≤ 400 + stenosis > 50%) had the highest rates of hospitalizations, percutaneous coronary interventions, and combined major adverse events (all p < 0.0001).
The overall higher resource utilization among patients with stenosis is partially explained by the fact that when physicians see a significant stenosis, they tend to perform more procedures than is the case with a high calcium score alone, which is more likely to generate additional tests rather than procedures, Chinnaiyan said.
That's one limitation of the study. Others include the retrospective design -- "and we didn't call patients to see how their lifestyle had been modified" after looking at the results, she said.
But the multivariable analysis of major adverse event predictors showed that "when you add stenosis severity, the calcium score falls out. It's really stenosis severity that drives everything, not calcium scores," she said.
 |
| At multivariate analysis, stenosis severity assessed by coronary CTA was the strongest independent predictor of major adverse cardiac events (all p < 0.0001). |
Importantly, all patients in the present study were symptomatic, with suspected coronary artery disease that caused a referral to coronary CTA in the first place. "In asymptomatic patients, we've learned over and over that calcium is a fantastic tool," she said.
New CAC study
A new University of California, Los Angeles (UCLA) study of 44,000 asymptomatic individuals who underwent calcium scans underscores the prognostic value of CAC in those individuals, Chinnaiyan said.
Budoff and colleagues found few deaths in individuals with zero calcium scores -- even in the presence of risk factors such as diabetes and smoking.
After a median follow-up of 5.6 years, there were just 104 deaths (0.52%) among the 19,898 patients (45%) without CAC on screening electron-beam tomography, compared to 58 deaths in those with CAC 1 to 10 (1.06%) and 739 deaths in those with CAC greater than 10 (3.96%), the researchers reported (Journal of the American College of Cardiology: Cardiovascular Imaging, June 2009, Vol. 2:6, pp. 692-700).
"In appropriately selected asymptomatic patients, the absence of CAC predicts excellent survival with 10-year event rates of approximately 1%," Budoff and colleagues concluded. "A finding of 0 CAC might be used as a rationale to emphasize lifestyle therapies rather than pharmacotherapy and to forgo repeated imaging studies."
CAC scoring at Beaumont
Calcium scores seem to get the patient's attention like nothing else, Chinnaiyan said.
"When we tell patients to do something, it may or may not get through," she said. "But when you have results of calcium score, suddenly their ears perk up and there is much more adherence" to pharmacologic therapies and positive lifestyle changes.
"But anytime you are trying to evaluate symptomatic patients, the calcium score is not predictive of anything," she said. For a while, in fact, the hospital stopped doing calcium scans routinely in symptomatic patients referred for coronary CTA.
But owing to the demonstrated long-term prognostic value of calcium, Chinnaiyan said, the physicians thought it best to restore the CAC test for now, even in symptomatic individuals.
Pending more long-term results, of course, performing coronary CTA in asymptomatic individuals "is considered an inappropriate indication regardless of baseline risk," she said. Last year a Chinese group reported their experience in 1,000 asymptomatic patients, and the "prevalence of disease was not enough to justify radiation and contrast dose," Chinnaiyan said.
This is a reality that probably won't change anytime soon, she said, "which is why we need long-term studies to see how we are affecting life span. Unless we have more data, we really can't advocate [coronary] CTA in asymptomatic patients."
Notwithstanding questions about improved survival and radiation dose, screening everyone at risk with coronary CTA "would be a huge burden to the healthcare system," she said. "We want to be cautious and proceed, making sure the data show we are saving lives."
By Eric Barnes
AuntMinnie.com staff writer
August 14, 2009
Related Reading
Dual-source CTA turns in mixed results for coronary stenoses, July 30, 2009
Coronary artery calcium independently predicts risk in CAD patients, July 29, 2009
Zero calcium means good outcomes, even with undetected plaques, July 23, 2009
CTA predicts coronary plaque instability, June 30, 2009
Absence of coronary calcium predicts excellent 10-year survival: study, June 18, 2009
Copyright © 2009 AuntMinnie.com