Cardiovascular MRI can be performed safely, with low risk and limited hemodynamic changes, on infants with congenital heart disease, according to a study conducted at the Heart and Diabetes Center in Bad Oeynhausen, Germany.
The lead author of the study was Dr. Samir Sarikouch from the center's department of congenital heart disease; Sarikouch and colleagues published research details from the study online in Pediatric Cardiology (August 15).
The retrospective study reviewed a total of 20 infant patients (13 boys and seven girls) with pre- and postoperative congenital heart defects in the facility's pediatric cardiac intensive care unit from January 2005 to December 2006. The infants had a mean age of 4.9 months, ranging from six days to 12 months old. Intracardiac malformations were present in 16 of the infants, with vascular rings causing tracheal stenosis evident in three patients.
All of the infants were referred for further MRI evaluation for congenital heart defects. In 18 of the 20 cases, transthoracic echocardiography could not visualize cardiovascular morphology sufficiently, while cardiac catheterization did not provide sufficient information for the other two patients.
All exams were conducted on a standard 1.5-tesla whole-body MRI scanner (Philips Healthcare, Andover, MA), using a two-element phased-array head and neck or a five-element cardiac coil.
Patient monitoring
The study also compared arterial blood pressure and heart rate before, during, and after the MRI exams and found no significant differences. The mean heart rate was 140 beats per minute before the MRI, 124 beats per minute during the MRI, and 140 beats per minute after the MRI.
In their analysis, the researchers also determined that cardiac MRI for an infant patient in the intensive care unit "has no delayed hemodynamic effects, as indicated by the evaluated parameters including serum lactate, diuresis, and the amount of diuretics up to 24 hours after the MRI."
The only exception was a 10-month-old girl receiving inotropic support who required a single dose of epinephrine after a breath-hold scan of 15 seconds, resulting in relative bradycardia, which resolved within 30 seconds. The study noted that her case "emphasizes the importance of complete hemodynamic monitoring during cardiac MRI for sick children."
Delicate transport
Transport of a critically ill infant also may involve risk, and hemodynamic stability should be optimized. Monitoring during transport is crucial. In the German study, the distance from the pediatric cardiac intensive care unit to the MRI and back to the intensive care unit was within a five-minute walk on the same floor. No complications occurred among the 20 patients during transport.
The mean time for the imaging procedures was 110 minutes, with a range of plus or minus 27 minutes. The calculation covered the time from the patient's arrival through intubation and positioning, the imaging scan, and the return to the pediatric cardiac intensive care unit. The researchers reported that all exams were completed successfully with good image quality.
The study noted that the "noninvasive nature of MRI and its great clinical impact on management decisions render cardiac MRI particularly attractive for patients with impaired hemodynamics for whom direct cardiac catheterization poses additional risks such as arrhythmias, infections, and contrast agent load."
 |
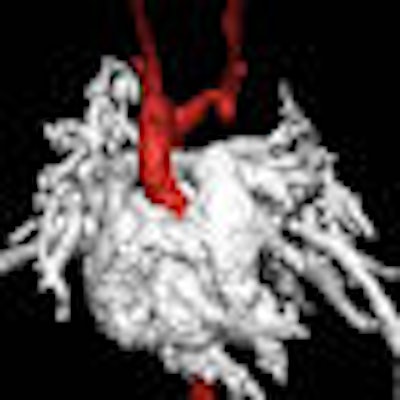
| This infant patient presented with tracheal stenosis due to a double aortic arch with an atretic left anterior part. Transverse turbo spin-echo images display the tracheal stenosis by the right aortic arch as seen in image A (top). A 3D volume-rendered reconstruction of the double aortic arch with the atretic left anterior arch is shown in image B (bottom). Each arch gives rise to the ipsilateral common carotid and subclavian artery. Images courtesy of Pediatric Cardiology. |
 |
CT's limitations
While cardiac CT is an effective method to delineate extracardiac vessel malformations and airway problems given its short acquisition time, the researchers cautioned that CT is "limited largely to morphologic assessment because no hemodynamic data can realistically be expected from CT with small children." In addition, smaller children's "up to 10-fold" sensitivity to radiation is a concern for infants with complex congenital heart disease.
Given CT's limitations, the authors noted that cardiovascular MRI is considered the "method of choice by many institutions when transthoracic echocardiography is inconclusive and the patient is stable enough to undergo a longer investigation under general anesthesia."
With no acute or delayed hemodynamic adverse effects and no significant intraprocedural complications from MRI, the researchers concluded that cardiovascular MRI "is safe and has important management implications even for this highly vulnerable patient group."
By Wayne Forrest
AuntMinnie.com staff writer
August 29, 2008
Related Reading
FDA posts pediatric imaging advisory, June 25, 2008
House resolution advocates lower pediatric x-ray dose, May 27, 2008
MRI edges out CT in postinfarct myocardial studies, May 8, 2008
Anesthesiologists refine pediatric sedation for MRI, October 25, 2007
Pediatric MRI and suite templates: If the shoe doesn't fit, don't wear it, April 25, 2006
Copyright © 2008 AuntMinnie.com