With experience and proper understanding of pitfalls such as artifacts, users can successfully handle 3D and 4D ultrasound studies, according to Dr. Dolores Pretorius of the 3D US Imaging Group at the University of California, San Diego.
Pretorius shared some practical advice for using 3D and 4D ultrasound during a talk at the 2005 Leading Edge in Diagnostic Ultrasound Conference, held in May in Atlantic City, NJ.
First, users need to keep in mind that 3D has better resolution than 4D, and that resolution quality must be optimized for the type of exam prior to the volume acquisition, she said.
"That means you have to make your 2D as good as you can," she said.
The transducer must be positioned over the organ in the optimal plane of acquisition, which varies depending on the application, Pretorius said. For example, the optimal plane for a face acquisition is the sagittal plane; the optimal plane for looking at the palate is the axial plane.
Magnification must also be optimized for 3D evaluation, she said.
"You have to watch when you buy equipment how to do (magnification)," Pretorius said. "It does make a difference."
For the 2D US scan performed prior to the 3D/4D study, set image gain a little greater than usual for 2D US, she said. The extra contrast is needed to produce the rendered pictures.
The 2D ultrasound scan should be used to identify the target and the best acquisition plane, the area with the most fluid and least overlying structures, Pretorius said. Third, scan in parallel planes over the region of interest (ROI), and place the transducer over the center of the target as the volume will be swept out equally on both sides of the initial viewing plane, she said.
The acquired image is 90 degrees to the scanning plane.
"It takes a little time to get used to (90 degrees)," she said.
Next, push the button to acquire the 3D volume. Look at multiplanar images for motion and any resolution problems. Then rotate the image into a standard orientation and scroll through the image planes, Pretorius said.
Orientation of the uterus is very important, she said. She suggests that two hands be used to scan, and that the fetal surface be positioned adjacent to fluid.
"You may need to 'push fluid' by tapping with finger of opposite scanning hand or pushing with whole hand," she said. "Consider gently pushing the fetus with the opposite hand."
Pretorius suggests rolling the patient to move fluid and baby away from the uterine wall. After the target is identified, hold the transducer steady and allow the fetus to move, she said. A relatively large ROI should be set in order to observe fetal movement.
"Most of the time people tell you to take a smaller region of interest because it allows better resolution, but if you're looking for movement, you need a big region of interest," she said.
Alternate between multiplanar and rendered images; it will be necessary to use the 2D image to guide the scanning for the 4D image, Pretorius said. The beam should be steered from various angles to optimize viewing of the volume.
"Beam steering from the posterior aspect of the uterus toward the front wall --180 degrees from the opposite of what you would expect -- may be very helpful in scanning limbs," she said.
For the rendering process, choose the ROI boundaries and set the boundaries to enable rendered image referencing, she said. Different vendors will have different ways of setting these boundaries, Pretorius said.
Users can display studies in a niche mode, and will need to choose from rendering options such as thresholding, rendering mode mix, and the chroma map, she said.
"When I can't get a good rendered image, most often if I change their threshold I will get the picture I want," Pretorius said. "So the first knob for me to think about when I'm not getting what I want is the threshold knob."
Other options include a Magic Cut or scalpel-type functionality, the ability to rotate on the y-axis, and the creation of cine loops.
Users must then decide whether to save the 3D volume original, 3D volume Cartesian, 3D cine, 2D screen, 2D cine, and 4D cine studies, and how they want to view them on the workstation, if they wish to do that, she said.
Artifacts
Of course, any practical discussion of 3D ultrasound requires understanding of the perils of artifacts, which may mimic abnormal development, masses, or missing structures. In fact, correct identification of artifacts is essential, Pretorius said.
"Any time you find anything from the rendered images, you need to confirm it on 2D and go back and look at your multiplanar images," she said.
Sources for 3D ultrasound artifacts can be B-mode artifacts (resolution, propagation, and attenuation matters), color or power Doppler artifacts (from aliasing and gain), and 3D ultrasound-specific artifacts from acquisition, rendering, and editing, Pretorius said.
Three-dimensional ultrasound-specific artifacts can be realized during the acquisition process from patient motion, such as respiration or fetal motion. Organ motion, such as vessel pulsations, cardiac motion, and peristalsis, can produce artifacts as well, she said.
 |
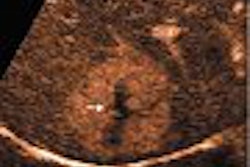
| Motion artifact simulating cleft lip in 32-week fetus. Image courtesy of Dr. Dolores Pretorius. |
Position-sensing errors can also have an impact. Metallic distortion can be produced by metal in the region of interest or in the area around your table if a magnetic sensor is being used to acquire the data, she said.
Improper calibration and operation will also produce poor data, Pretorius said. In addition, a lack of position-sensing capability on equipment can lead to improper geometry assumptions.
Rendering can also introduce artifacts, owing to too much or too little thresholding, as well as ROI boundaries artifacts. For example, an ROI boundary placed across the head would make it appear as if the baby has a hole in the head.
In addition, the editing process can lead to deletion of volume data that shouldn't be deleted, she said.
By Erik L. Ridley
AuntMinnie.com staff writer
August 12, 2005
Related Reading
3D offers speed gains for fetal scanning, July 1, 2005
AMA says ultrasound in-utero 'portraits' are bad idea, June 22, 2005
4D ultrasound shows promise for improving fetal echocardiography, April 6, 2005
3D volume US shows promise for second-trimester fetal evaluation, March 17, 2005
3D ultrasound poised to revolutionize pelvic imaging, September 9, 2004
Copyright © 2005 AuntMinnie.com