Non-Hodgkins Lymphoma:
View images of Non-Hodgkins lymphoma
Clinical:
Non-Hodgkins lymphomas (NHL) account for nearly 80% of lymphomas. The incidence of NHL is rising, in part due to the increased incidence of this tumor in HIV patients. Although the tumor can occur at any age, affected patients are usually older with a median age of 55 years [2].
Non-Hodgkins lymphomas are staged according to the NIH classification as either: 1- Follicluar or Diffuse; 2- Small or Large cell; and 3- Cleaved or Un-Cleaved (ie: a tumor may be classified as a follicular, cleaved, small cell lymphoma). Tumors are considered to be follicular if the lesion remains contained within nodular areas within the involved nodes. Diffuse lesions lack this nodular characteristic, and are dispersed throughout the involved node. Follicular, cleaved cell, and small cell lesions are generally less aggressive (ie: low grade). Although indolent, low grade lesions are generally also more difficult to cure. Overall, prognosis is much worse than for Hodgkins lymphoma with a 5 year cure of approximately 40%. Diffuse large cell lymphoma in particular can disseminate rapidly to the lungs.
X-ray:
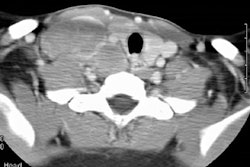
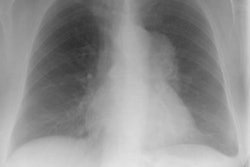
Non-Hodgkins presenting as a mediastinal mass is less common (about 20% of cases) than Hodgkins and other areas of adenopathy are also usually seen. The most common NHL's to involve the mediastinum are large B-cell lymphoma and lymphoblastic lymphoma [2]. Lung parenchymal involvement at presentation is found in less than 5% of cases, but pulmonary involvement can occur without associated mediastinal/hilar adenopathy. The radiographic patterns of parenchymal involvement are identical to those seen in Hodgkin's disease and again, multiple nodules are the most common finding (Note: AJR 1997; 168: p 340- these authors state that the most common radiographic finding in primary non-Hodgkins lymphoma of the lung is an area of poorly defined opacification with air bronchograms). Less common findings include bilateral air space consolidation and segmental or lobar atelectasis.
The
CT angiogram sign (visualization of an enhancing vessel within the area
of consolidated
lung), which is characteristically described in association with
bronchoalveolar cell
carcinoma, may also be seen with primary pulmonary lymphoma. Cavitation
of nodules is rare
prior to treatment.
Pleural involvement is rare, but pleural effusion is common and tend
to be reactive and related to proximal lymphatic obstruction from nodal
disease [5]. A pericardial effusion, if present, is typically malignant
[5].
Calcification is found in less than 1% of cases prior to treatment, but may suggest a more aggressive lesion [4]. Calcification can be seen in 2-8% of cases after treatment with radiation or chemotherapy [4].
CT cannot be used to monitor response to treatment as residual abnormalities are frequently detected and may represent non-viable fibrotic tissue [3].
Scintigraphy in Non-Hodgkins: Gallium sensitivity is reported to be better than 85% for high grade tumors, and is particularly good for histiocytic lymphoma (89%). Sensitivity for low grade (slow growing) tumors is poor, although these patients tend to have a more favorable prognosis. Scinitgraphy can be used to monitor response to treatment [3].
Thallium imaging can add useful information in the evaluation of Non-Hodgkin's lymphoma. Thallium generally has a higher avidity for low grade lymphomas than gallium, while its uptake in high grade lesions is usually poor (approximately 25% of low grade lymphomas are thallium positive and gallium negative. Due to gut activity, thallium imaging is not useful for the evaluation of abdominal or pelvic disease.
PET: See PET imaging section for additional information
REFERENCES:
(1) AJR 1997; Au V, Leung AN. Radiologic manifestations of lymphoma in the thorax. 168: 93-98 (No abstract available)
(2) Chest 1997; Strollo DC, et al. Primary mediastinal tumors. Part II. Tumors of the middle and posterior mediastinum. 112: 1344-57
(3) Radiology 2000; Front D, et al. Aggressive non-Hodgkin lymphoma: Early prediction of outcome with Ga67 scintigraphy. 214: 253-257
(4) AJR 2002; Apter S, et al. Calcification in lymphoma occurring
before
therapy: CT features and clinical correlation. 178: 935-938
(5) AJR 2011; Thomas AG, et al. Extranodal lymphoma from head to
toe: Part 2, the trunk and extremities. 197: 357-364