Aspiration Pneumonia:
Clinical:
Patients with altered consciousness or impaired cough and swallowing reflexes are an increased risk for aspiration. In the supine patient the aspiration will typically involve the posterior segments of the upper lobes and the superior segments of the lower lobes. In an upright patient, the lung bases tend to be primarily involved- espacially the right lower and middle lobes due to the more vertical course of the right main bronchus compared to the left side [5]. The main complications of aspiration are: 1- a chemical pneumonitis due to sterile gastric contents; 2- a pneumonia due to aspirated pathogenic bacteria from the oropharynx; and 3- airway obstruction due to aspiration of solids. Symptoms acute aspiration with chemical pneumonitis include apnea, cyanosis, hypotension, fever, and rales or wheezing on physical exam. Leukocytosis with a left shift may be observed.Although there is no specific threshold, lung injury increases significantly as the volume of aspirate increases. Lower pH (greater acidity) of the aspirated material is also associated with an increased risk of lung injury. A pH of greater than 2.5 usually will not produce significant injury. Acid secretions damage the alveolar lining producing a chemical pneumonitis. There is reduced surfactant and this leads to increased permeability pulmonary edema (or hemorrhagic pulmonary edema) [4].
Regardless of the pH, aspiration of food contents is associated with a greater likelihood for lung injury. Organisms within the aspirate (typically anaerobic species) can result in superinfection. Recurrent aspiration can lead to a range of pulmonary complications including asthma, chronic bronchitis, bronchiectasis, and pulmonary fibrosis.
X-ray:
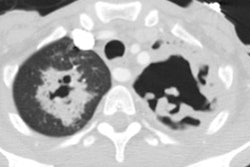
Radiographically, minor aspiration or early films may fail to produce any findings. Consolidation is the most common finding and represents a chemical pneumonitis. Findings are bilateral in up to 70% of patients. Consolidation may progress rapidly to become a diffuse process- especially in acute aspiration of massive amounts of gastric acid with a pH of less than 2.5. The radiologic abnormalities tend to worsen for several days and then improve quickly, unless there is a superimposed bacterial pneumonia or ARDS. Aspiration of partially digested food usually results in small, localized abnormalities due to atelectasis distal to the airway obstruction. Findings typically clear quickly (24-48 hours) as mucociliary action and coughing clear the airway. Persistent opacities for more than 4 to 5 days suggest a superimposed infection [3]In mild aspiration, CT may show tree-in-bud opacities that would be undetected on CXR [5].REFERENCES:
(1) Radiol Clin North Am 1996 Jan;34(1):83-96
(2) ACR Syllabus #40: p.375-77
(3) AJR 1999; Marom EM, et al. The many faces of pulmonary aspiration. 172: 121-128
(4) AJR 2008; Kim M, et al. MDCT evaluation of foreign bodies and
liquid aspiration pneumonia in adults. 190: 907-915
(5) AJR 2013; Nemec SF, et al. Lower lobe-predominant diseases of
the lung. 200: 712-728