Lung Abscess:
Clinical:
Lung abscesses typically occur as a complication of a necrotizing pulmonary infection- particularly S. aureus, Klebsiella, or from aspiration of anaerobic oropharyngeal bacteria (ie: in patients with altered consciousness, gastroesophageal dysmotility or poor dental hygiene). Patients present with cough, fever, sputum production, chest pain, and hemoptysis. Complications include spillage of infected fluid into the tracheobronchial tree with spread of infection, bronchopleural fistula formation, hematogenous dissemination, and hemorrhage/hemoptysis. Hemoptysis occurs in between 10 to 15% of patients with lung abscesses and may be life-threatening in nearly half of these cases.Most lung abscesses (80-90%) with resolve with medical management consisting of antibiotics and postural drainage. Those which fail to respond to this regimen are generally associated with an obstructed bronchus and management becomes surgical. Other indications for intervention include persistent sepsis, hemoptysis, or development of bronchopleurofistula and empyema. Percutaneous drainage with an 8 to 14 Fr catheter may be performed- it is effective and has low associated morbidity. The catheter should be placed through areas of abnormal lung and pleura to decrease the risk of producing an empyema or bronchopleural fistula. If there is no other route to the abscess than through normal lung, then this principal may be violated and in most cases there are no serious sequella [2].
X-ray:
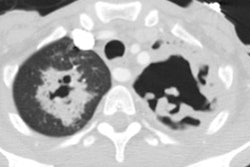
On CXR a lung abscess classically appears as a cavitary lesions containing an air-fluid level and there is a surrounding rim of lung tissue. The wall thickness of a lung abscess progresses from thick to thin, and ill-defined to well circumscribed as the surrounding lung infection resolves. The wall can be smooth or shaggy, but is less commonly nodular (which suggests a cavitary carcinoma). The air-fluid level contained within a lung abscess is usually of equal length on orthogonal views. If the abnormality extends to the pleural surface, the borders of the abscess classically form acute angles with the chest wall.On CT an abscess is often rounded with a relatively thick wall and ill-defined, shaggy margin. Vessels and bronchi are not displaced by the lesion as they are by an empyema, in fact, lung markings go into the lesion. The epicenter of an abscess is within the parenchyma. The lesion will usually form acute angles with the chest wall if extends to the pleural surface.
REFERENCES:
(1) AJR 1995; Klein JS. Interventional radiology of the chest: Image-guided percutaneous drainage of pleural effusions, lung abscess, and pneumothorax. 164: 581-588
(2) J Thorac Imaging 1998; van Sonnenberg E, et al. Percutaneous drainage of thoracic collections.13: 74-82
(3) Radiol Clin N Am 2005; Tarver RD, et al. Radiology of community-acquired pneumonia. 43: 497-512